
Michelle Lyons is instructor of "Oncology and the Female Pelvic Floor: Female Reproductive and Gynecologic Cancers", among other Herman & Wallace courses. We thought you might like to hear her expert analysis of current research going on in the field of gynecologic oncology, and the benefits therapeutic yoga can have on patient rehabilitation. Take it away, Michelle!

More than 65,000 women are diagnosed with gynecologic cancers (vulvar, vaginal, cervical, ovarian, endometrial) in the United States each year (Sohl et al 2012). Treatment options for these women include surgery, chemotherapy, radiation and hormone therapy – all of which have the potential to have local, regional and global effects on a woman’s body. The pelvic rehab specialist is in a unique position to hugely improve quality of life issues for these women – dealing with issues directly associated with pelvic health (urinary, sexual and bowel function and dysfunction) as well as more global issues such as bone health, peripheral neuropathies and musculoskeletal dysfunctions.
Yoga has enormous potential as a therapeutic tool for gynecologic cancer survivors and as exercise prescription experts, we can add yoga as a multi-purpose tool to our skill-set.
Empirical research on therapeutic yoga has been ongoing for several decades, including several recent studies conducted with cancer patients and survivors. Although most of the research looking at the benefits of yoga for cancer survivors has been done in the context of breast and prostate cancers, we can safely extrapolate many of the benefits associated with oncology rehab yoga, including its immediately obvious ability to improve flexibility, strength, balance, but also the impact yoga can have on decreasing inflammation, improving sleep and raising quality of life scores in pelvic cancer survivors.
Recent papers by Dewhirst et al showed how moderate exercise can improve the efficacy of chemotherapy and radiation by decreasing tumour hypoxia – they also discovered that this may limit metastatic aggression.
We also know that exercise can be potent medicine when it comes to dealing with the effects of cancer treatments, especially fatigue, bone health and cardiovascular function, which may disrupt return to exercise (Kerry et al 2005). But pelvic cancer patients may face extra barriers when it comes to returning to exercise, such as pelvic pain and concerns about continence, as well as diminished flexibility, balance and strength. But as Blaney et al concluded in their 2013 paper ‘…however, the main barriers reported were those that had the potential to be alleviated by exercise.’ And in my opinion, this can be achieved by integrating yoga into our pelvic oncology rehab programs.
These recent and exciting research findings have encouraged me to add a therapeutic yoga lab session to my Oncology & the Pelvic Floor course, which I will be teaching in NY next month. This is the last chance to catch this course stateside this year so I hope you will join me in White Plains to explore the many ways we can make a serious impact on pelvic cancer survivorship (Bring your yoga mat!)
References:
Psychooncology. 2013 Jan;22(1):186-94.
Cancer survivors' exercise barriers, facilitators and preferences in the context of fatigue, quality of life and physical activity participation: a questionnaire-survey. Blaney JM1, Lowe-Strong A, Rankin-Watt J, Campbell A, Gracey JH.
Annals of Behavioral Medicine
April 2005, Volume 29, Issue 2, pp 147-153
A Longitudinal Study of Exercise Barriers in Colorectal Cancer Survivors Participating in a Randomized Controlled Trial
Kerry S. Courneya Ph.D., Christine M. Friedenreich Ph.D., H. Arthur Quinney Ph.D., Anthony L. A. Fields M.D., Lee W. Jones Ph.D., Jeffrey K. H. Vallance M.A., Adrian S. Fairey M.Sc.
JNCI J Natl Canc
Allison S. Betof, Christopher D. Lascola, Douglas H. Weitzel, Chelsea D. Landon, Peter M. Scarbrough, Gayathri R. Devi, Gregory M. Palmer, Lee W. Jones, and Mark W. Dewhirst
Modulation of Murine Breast Tumor Vascularity, Hypoxia, and Chemotherapeutic Response by Exercise
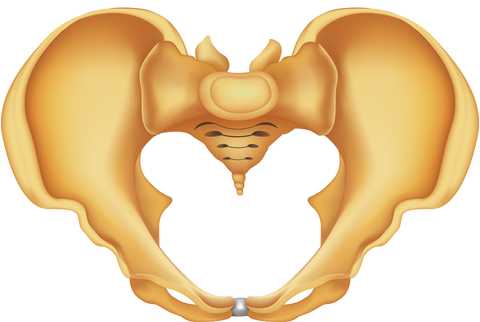
Pelvic rehabilitation providers commonly treat a variety of conditions associated with peripartum pelvic girdle dysfunction. This list of conditions includes coccyx pain, and a recent study aimed to identify risk factors which may lead to coccyx pain in the postpartum period. Dr. Jean-Yves Maigne, who is well known for providing foundational research on the topic of coccyx pain, and colleagues completed a case series of 57 postpartum women presenting to a specialty coccydynia clinic. Dynamic x-rays were taken to assess mobility of the coccyx, and data about delivery methods were collected. (A control group of 192 women were comprised of women who also presented to the clinic but who had coccyx pain from other causes.)

The authors found that the women reported immediate postpartum pain in the coccyx with sitting. Instrumentation was a common finding in regards to the patients’ deliveries. 50.8% of the deliveries utilized forceps while 7% were vacuum-assisted. An additional 12.3% of the deliveries were spontaneous and were described as “difficult.” A subluxation of the coccyx was observed in 44% of the women who developed coccyx pain after childbirth as compared to 17% of the controls. A fractured coccyx occurred in 5.3 % of the women. Body mass index (BMI) of more than 27 and having 2 or more vaginal deliveries was also associated with a higher prevalence of a subluxation of the coccyx.
Being unable to sit comfortably following childbirth could make a new parent’s life very difficult with limitations in activities such as sitting to feed the baby. Socially, being unable to sit comfortably can also limit many activities. The women in this study reported immediate tailbone pain with sitting, which can alert providers to a condition requiring both immediate and follow-up attention. Risk factors such as having a difficult delivery or use of forceps may also signal a patient history that may lead to coccyx pain.
If you are interested in learning more about managing coccyx pain, join Lila Abbate at Coccyx Pain Evaluation and Treatment in Bay Shore, NY on October 25-26! You may also be interested to learn more about treating patients during the postpartum period, in which case Care of the Postpartum Patient is right up your alley!

Today we get the opportunity to hear from Herman & Wallace faculty member Elizabeth Hampton PT, WCS, BCIA-PMB! Elizabeth has been kind enough to offer her insights about the diagnosis of pelvic rehabilitation patients. Join Elizabeth at Finding the Driver in Pelvic Pain this November in Houston, TX in order to learn evaluation tools for complex pelvic pain clients!
 Having taught for Herman and Wallace since 2006, I have a few observations that have been consistent over the years. Clinicians want their clients to get better, so much so that they are ready to jump in to treatment before having a solid problem list and validated findings. I can understand this: after a 3 day course we have clients Monday morning at 8 a.m. who have been waiting for us to take this course so we can get them better! We had better be smart ASAP! But what do we do when we are treating symptoms rather than understanding the primary, secondary and tertiary factors in their condition?
Having taught for Herman and Wallace since 2006, I have a few observations that have been consistent over the years. Clinicians want their clients to get better, so much so that they are ready to jump in to treatment before having a solid problem list and validated findings. I can understand this: after a 3 day course we have clients Monday morning at 8 a.m. who have been waiting for us to take this course so we can get them better! We had better be smart ASAP! But what do we do when we are treating symptoms rather than understanding the primary, secondary and tertiary factors in their condition?
Finding the Driver in Pelvic Pain is a course that is a foundational first step in screening the pelvic pain client. It is a great place to start. I developed the course because there was no evidence based comprehensive factors that had been established as fundamentals for screening a pelvic pain client.
The other thing I have learned after teaching Pelvic Floor Function, Dysfunction, & Treatment – Level 2B for 9 years is that the majority of clinicians who take this intermediate level course cannot perform a precise vulvar and intrapelvic muscle mapping assessment. Close your eyes and pretend you are mapping a client’s left iliococcygeus: can you place your finger in the proper orientation and know 100% you would be palpating it? Indeed, this takes training and repetition. Internal pelvic floor muscle mapping is a key part of the Finding the Driver screening system.
What do you do when you have a pelvic pain client on your schedule and a 45-60 minute slot? How do you screen findings and get the plan of care within such a short period of time? Finding the Driver is a comprehensive pelvic floor and musculoskeletal screening to rule in or rule out drivers of the pain from all sources including spine, pelvic ring, neural entrapment, intra-articular hip, load transfer, biomechanics and motor control. There is a clear flow to the screening process and an emphasis on how to organize that information, as we know with pelvic pain, it is the copious amount of information that is the challenge. We have two case studies with either participants or clients of a local Physical Therapist who come in and we go through the entire screen, prioritize treatment and provide that treatment during the course. The participants walk away with clear clinical reasoning for their treatment and prioritization of treatment as primary, secondary, and so on. The goal of the course is to help the clinician sort through the extraordinary amount of information we gather on our pelvic pain client and organize it in a way that we can explain to the client as well as create our plan of care. Treatment is not linear, as we are frequently treating many aspects at the same time. However being able to organize the information is key in designing that plan of care. For example, with a prone knee bend that reproduces labial pain, we find that the genitofemoral nerve is causing referred pain. However that referral may be due to constipation, irritable bowel, inguinal entrapment due to hernia surgery, intra-abdominal adhesions due to endometriosis, osteitis pubis or facilitated segment at the upper lumbar spine. How do we tease that out? How do you sequence nerve glide, visceral work, soft tissue mobilization, joint mobilization and dietary components for colonic motility? The treatment with all of those components are very different indeed. Finding the Driver is a hands on course with systematic screening tools and, with case studies, we go through treatments appropriate to that client. The focus is on what we, as physical therapists, can do to understand the drivers.
At the last Finding the Driver course in Milwaukee, WI, we had two case studies in pelvic pain. One client reported chronic psoas and adductor tightness with deep left sided pelvic pain. As a professional aerialist, she was extraordinarily flexible and demonstrated positions of tightness that concerned her, which included lateral splits with her hips in slight horizontal abduction and extension (yes, yikes!) When she reported that her adductor felt tight in this position, I explained it was because it was trying to keep her leg attached to her body! She was 9/9 on the Beighton scale and had severe multidirectional instability in her hips, impaired load transfer through her pelvis, respiratory dysfunction with efforts at pelvic floor and transverse abdominis contraction, as well as repeated choice of activities that were profoundly provoking. Interestingly, she was better at load transfer during handstands (bilateral or unilateral) vs. in standing and we discussed her course of treatment addressing the primary, secondary and tertiary aspects of her condition. Another client had severe labial pain, and despite multiple abdominal and intravaginal surgeries, her symptom onset was 4 months prior. She certainly had visceral, postural, joint restrictions, movement dysfunction and many other factors. But her primary driver was a labral tear in her hip and she needed surgery. After surgery, her pain was 100% resolved and in her post op rehab, the other factors could be addressed.
It is safe to say that it can be difficult to perform a comprehensive screen in 45-60 minutes on ALL clients. We all know that many of our clients need to tell their story and because of fear or previous negative history, we may choose as clinicians how to spend that session to best honor the needs of the client. That being said, Finding the Driver is a course which provides a solid start in differential diagnosis so you can drill down into more specifics on subsequent visits.

Today we present Part II of Michelle Lyons' discussion on sex after gynecologic cancer. Michelle will be teaching a course on this topic in White Plains in August!
In Part One of this blog, I looked at the sexual health issues women face after gynecologic cancer. In Part Two, I want to explore different treatment options that we as pelvic rehab specialists can employ to help address the many implications of cancer and cancer treatment
Treatment for gynecologic cancers, including vulvar, vaginal, cervical, endometrial and ovarian cancers, may include surgery, radiation therapy, chemotherapy, and/or hormonal therapy. We know that any of these approaches can have an adverse effect on the pelvic floor, as well as systemic effects on a woman’s body. Issues can include pain, fibrosis, scar tissue adhesions, diminished flexibility, fatigue and feeling fatigued and unwell. The effects on body image should not be under-estimated either. In their paper ‘Sexual functioning among breast cancer, gynecologic cancer, and healthy women’, Anderson & Jochimsen explore how ‘…body-image disruption may be a prevalent problem for gynecologic cancer patients…more so than for breast cancer patients’. The judicious use of manual therapy and local and global exercise prescription may be excellent pathways for a women to re-integrate with her body.
Many women will have to learn to care for a new colostomy or how to catheterize a continent urostomy. A woman who has had a vulvectomy will need sensitive counselling to understand that she can still respond sexually. Patients who have had a vaginectomy with reconstruction as part of a pelvic exenteration will need extensive rehab to help them achieve successful sexual functioning. We as pelvic rehab practitioners are in a uniquely privileged position – not only can we ask the questions and discuss the options but we are licensed to be ‘hands on’ professionals, using our core skills of manual therapy, bespoke exercise advice and educating our patients about a range of issues from the correct usage of lubricants, dilators, sexual ergonomics and brain/pain science. I am in the habit of describing pelvic rehab as the best specialty in physical therapy but I think this is especially true when it comes to the junction of oncology and pelvic health. This is where we can integrate our knowledge of neuro-science, orthopaedics, the lymphatic system and pelvic health to deal with the effects of pelvic cancers and their treatment.
In Farmer et al’s 2014 paper, ‘Pain Reduces Sexual Motivation in Female But Not Male Mice’ , the authors found that ‘Pain from inflammation greatly reduced sexual motivation in female mice in heat -- but had no such effect on male mice’. Unfortunately ongoing pelvic pain is a common sequela of treatment for gynecologic cancers – reasons ranging from post-operative adhesions, post-radiation fibrosis or vaginal stenosis or genital lymphedema. It is also worth bearing in mind the ‘rare but real’ scenario of pudendal neuralgia following pelvic radiation, as discussed by Elahi in his 2013 article ‘Pudendal entrapment neuropathy: a rare complication of pelvic radiation therapy.’
The good news is that we have much to offer. Yang in 2012 (‘Effect of a pelvic floor muscle training program on gynecologic cancer survivors with pelvic floor dysfunction: A randomized controlled trial’) showed that pelvic rehab improved overall pelvic floor function, sexual functioning and QoL measures for gynecological cancer patients. Yang’s pelvic rehab group (administered by an experience physiotherapist) displayed statistically significant differences in physical function, pain, sexual worry, sexual activity, and sexual/vaginal function. Gynecological cancer and treatment procedures are potentially a fourfold assault: on sexual health, body image, sexual functioning, and fertility. Sexual morbidity is an undertreated problem in gynecological cancer survivorship that is known to occur early and to persist beyond the period of recovery (Reis et al 2010). We have a good and growing body of evidence that pelvic rehab, delivered by skilled therapists, has the potential to address each of these issues. And perhaps, most encouraging, here is Yang’s conclusion: ‘…‘Pelvic Floor Rehab is effective even in gynecological cancer survivors who need it most.’ (Yang 2012)
Interested in learning more about the role of pelvic rehab in gynecologic cancer survivorship? Join me in White Plains in August!
All Upcoming Continuing Education Courses

Pelvic Function Level 2B - Satellite - Mission Hills CA - May 19 - 20 2024
May 19 2024 - May 20 2024











Pelvic Function Level 1 - Satellite - Frankfort IL - June 1 - 2 2024 - SOLD OUT
Jun 1 2024 - Jun 2 2024


Pelvic Function Level 1 - Satellite - Columbus OH - June 1 - 2 2024 - SOLD OUT
Jun 1 2024 - Jun 2 2024


Mobilization of the Myofascial Layer Satellite Lab Course - Self-Hosted - June 7 - 9 2024
Jun 7 2024 - Jun 9 2024

Dry Needling and Pelvic Health - In Person - 3 - Day - Lake Stevens WA - June 7 - 9 2024
Jun 7 2024 - Jun 9 2024

Mobilization of the Myofascial Layer Satellite Lab Course - Kerrville TX - June 7 - 9 2024
Jun 7 2024 - Jun 9 2024

Mobilization of the Myofascial Layer Satellite Lab Course - East Greenwich RI - June 7 - 9 2024
Jun 7 2024 - Jun 9 2024

Mobilization of the Myofascial Layer Satellite Lab Course - Conyers GA - June 7 - 9 2024
Jun 7 2024 - Jun 9 2024

Mobilization of the Myofascial Layer Satellite Lab Course - Medford OR - June 7 - 9 2024
Jun 7 2024 - Jun 9 2024

Mobilization of the Myofascial Layer Satellite Lab Course - Houston TX - June 7 - 9 2024
Jun 7 2024 - Jun 9 2024


Pelvic Function Level 1 - In-Person - New Haven CT - June 8 - 9 2024 - SOLD OUT
Jun 8 2024 - Jun 9 2024







Pelvic Function Level 2B - Satellite - St. Petersburg FL - June 22 - 23 2024
Jun 22 2024 - Jun 23 2024


Pelvic Function Level 1 - Satellite - Greensboro NC - June 29 - 30 2024 - SOLD OUT
Jun 29 2024 - Jun 30 2024



Pelvic Function Level 1 - Satellite - Torrance CA - July 13 - 14 2024 - SOLD OUT
Jul 13 2024 - Jul 14 2024

Pelvic Function Level 1 - Satellite - Philadelphia PA - July 13 - 14 2024 - SOLD OUT
Jul 13 2024 - Jul 14 2024

Pelvic Function Level 1 - Satellite - San Diego CA - July 13 - 14 2024 - SOLD OUT
Jul 13 2024 - Jul 14 2024

Modalities and Pelvic Function - In Person - Raleigh NC - July 13 - 14 2024
Jul 13 2024 - Jul 14 2024