Can Vaginal Birth After Cesarean Success Be Predicted?

When a woman is interested in a trial of labor after previous cesarean delivery (TOLAC), she and her health care providers will consider the pros and cons of delivery methods. Researchers have aimed to predict success with vaginal birth after cesarean section (CS), with the intention of limiting the risk factors for both the mother and the fetus. A failed trial of labor following a CS may be associated with higher maternal and perinatal morbidity, according to the American College of Obstetricians and Gynecologists (ACOG) practice bulletin.
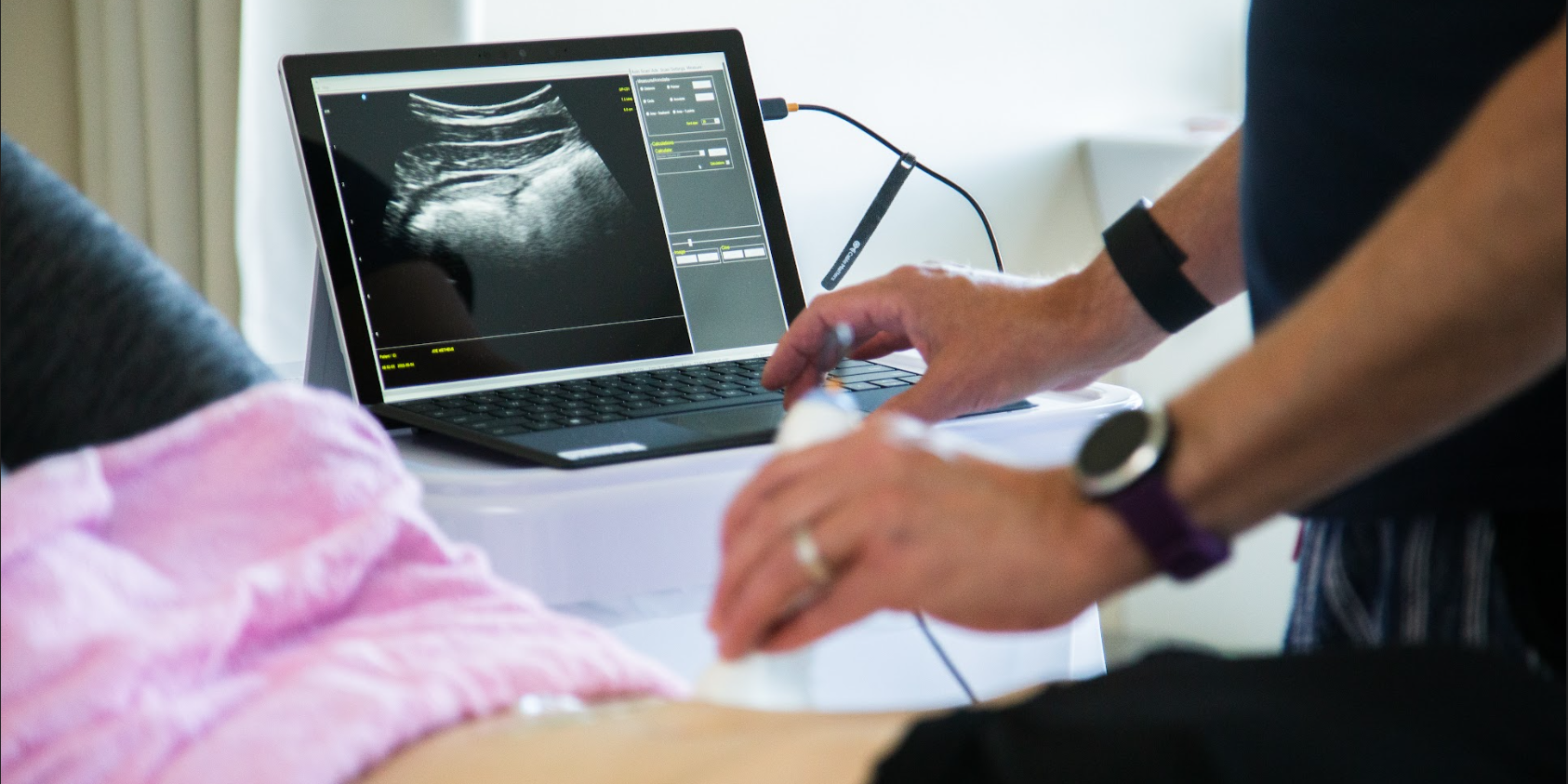
The goal of a study published last year was to develop a model for predicting success in women desiring a vaginal birth after cesarean (VBAC) section. All women had one prior CS, all were carrying singletons. Transvaginal ultrasound was utilized to evaluate the Cesarean scar (CS) at 11-13, 19-21, and 34-36 weeks' gestation in 320 women. The measurement of the scar was termed residual myometrial thickness (RMT), and the measurements also included the change in RMT from the 1st to 2nd trimester. With increased evidence that CS healing and myometrial thickness in the lower uterus may improve success with VBAC, this study is the first to assess scar dimensions across the first and second trimesters.
The CS scar was visible in 89% of the women. Of these, 153 of the 284 were excluded from the prediction model development due to having had more than one prior cesarean delivery, so the hospital protocol of scheduling cesarean was followed. The remaining women were offered a vaginal birth trial, with 10 of the 131 undergoing CS prior to labor for varied reasons. The final count of women included in the analysis was 121, and of these cases, 74 had successful VBAC, 47 experience failed trials of labor, primarily due to fetal distress, failure to progress, or possible scar rupture. (In the women who did not have a visible scar, 82% had a successful vaginal delivery.)
The median residual myometrial thickness, or RMT, was higher in patients who had a successful VBAC. Clinical usefulness, according to the study, is that use of the model may lead to fewer emergency CS deliveries through identification of women who will be successful with VBAC.
The authors concluded that measurements of a CS, when applied to a mathematical model, can predict success of a vaginal birth after CS. This information may be very interesting to discuss with our referring providers, our colleagues, as well as our patients. Any research that sheds light on variables to predict success with a VBAC may promote vaginal deliveries and hopefully prevent emergency cesarean deliveries. Educating our patients so they can be more informed and advocate for themselves is a key role. While we are always mindful of not overstepping our scope of practice, such as advising a woman if she should choose one method of delivery over another, the information about the scar thickness in predicting VBAC success may be very useful to both her and providers. For more information about peripartum issues, check out our Peripartum Course Series on the course page. There is still time to sign up for the Care of the Postpartum Patient continuing education course later this month in Chicago!
By accepting you will be accessing a service provided by a third-party external to https://www.hermanwallace.com/
All Upcoming Continuing Education Courses
Rehabilitative Ultrasound Imaging: Pelvic Health Satellite Lab Course - Self-Hosted - April 19 - 21 2024 - SOLD OUT
Apr 19 2024 - Apr 21 2024
Rehabilitative Ultrasound: Orthopedic Topics Satellite Lab Course - Self-Hosted - April 19 - 20 2024
Apr 19 2024 - Apr 20 2024

Parkinson Disease and Pelvic Rehabilitation - Remote Course - April 19 - 20 2024
Apr 19 2024 - Apr 20 2024

Rehabilitative Ultrasound Imaging: Orthopedic Topics Satellite Lab Course - Cedar Knolls NJ - April 19 - 20 2024
Apr 19 2024 - Apr 20 2024
Rehabilitative Ultrasound Imaging: Pelvic Health Satellite Lab Course - Cedar Knolls NJ - April 19 - 21 2024
Apr 19 2024 - Apr 21 2024


Pelvic Function Level 2C - Satellite - Torrance CA - April 20 - 21 2024 - SOLD OUT
Apr 20 2024 - Apr 21 2024



Pelvic Function Level 2C - Satellite - Springfield MO - April 20 - 21 2024
Apr 20 2024 - Apr 21 2024

Pelvic Function Level 1 - Satellite - New Bern NC - April 20 - 21 2024 - SOLD OUT
Apr 20 2024 - Apr 21 2024


Pelvic Function Level 1 - Satellite - Arlington VA - April 20 - 21 2024 - SOLD OUT
Apr 20 2024 - Apr 21 2024


Pelvic Function Level 1 - Satellite - Omaha NE - April 20 - 21 2024 - SOLD OUT
Apr 20 2024 - Apr 21 2024

Pelvic Function Level 1 - Satellite - Bedford NH - April 20 - 21 2024 - SOLD OUT
Apr 20 2024 - Apr 21 2024

Pelvic Function Level 1 - Satellite - Leavenworth KS - April 20 - 21 2024 - SOLD OUT
Apr 20 2024 - Apr 21 2024

Pelvic Function Level 1 - Satellite - Boston MA - April 20 - 21 2024 - SOLD OUT
Apr 20 2024 - Apr 21 2024

Pelvic Function Level 2B - Satellite - Seattle WA - April 27 - 28 2024 SOLD OUT
Apr 27 2024 - Apr 28 2024



Pelvic Function Level 2B - Satellite - Cranford NJ - April 27 - 28 2024 - SOLD OUT
Apr 27 2024 - Apr 28 2024

Menopause Transitions and Pelvic Rehab - Remote Course - April 27 - 28 2024
Apr 27 2024 - Apr 28 2024

Nutrition Perspectives for the Pelvic Rehab Therapist - Remote Course - April 27 - 28 2024
Apr 27 2024 - Apr 28 2024


Pelvic Function Level 2B - Satellite - Des Plaines IL - April 27 - 28 2024
Apr 27 2024 - Apr 28 2024



Pelvic Function Level 2B - Satellite - Hilton Head SC - April 27 - 28 2024
Apr 27 2024 - Apr 28 2024












Pelvic Function Level 1 - Satellite - Kankakee IL - May 4 - 5 2024 - SOLD OUT
May 4 2024 - May 5 2024