
This week The Pelvic Rehab Report sat down with faculty member Ken McGee, PT, DPT. Ken (they/he) is a queer transmasculine pelvic health physical therapist based in Seattle whose mission is to bring greater awareness to the pelvic health needs of the LGBTQIA2S community. Their practice, B3 Physical Therapy, centers on transgender and perinatal rehabilitation. Ken also provides peer bodyfeeding support and doula care, and can be found on Instagram at @b3ptcob3ptco.
You can join Ken in their remote course, Perinatal Mental Health: The Role of the Pelvic Rehab Therapist, scheduled for October 22, 2022.
Who are you? Describe your clinical practice.
Experiencing inadequate care for my own pelvic health conditions as a teenager motivated me to become a pelvic health physical therapist. Being a member of the queer community further drove me to offer trauma-informed care and develop better access to care through home visits. Currently, I split my time between providing gender-affirming physical therapy and serving as a birth doula.
What lesson have you learned (in a course, from an instructor, or from a colleague or mentor) that has stayed with you?
Very few clients will remember detailed biomechanical explanations or every exercise you teach them. However, each client will remember how you treated them and how you made them feel. Asking clients about their preferences for care and following up go a long way in establishing rapport.
What do you find is the most useful resource for your practice?
One of my favorite resources is Decolonizing Fitness. It is an educational platform by Ilya Parker, PTA, (he/they). It provides a catalog of exercises and trainings for people looking to improve their care of gender-diverse people and People of Global Majority.
What books or articles have impacted you as a clinician?
The healthcare field regularly puts people in boxes to determine care. For example, many providers might determine care based on whether someone is a transgender woman or man. However, gender is actually someone’s individual experience rather than a category. Kate Bornstein’s My New Gender Workbook is a good starting point for understanding gender as uniquely one’s own, rather than part of a treatment algorithm.
What made you want to create this course, Perinatal Mental Health?
I wanted to create this course because, as a parent and physical therapist, I see both the challenges that the perinatal period presents, as well as the ways that rehabilitation providers can support mental health. In developing the content, I drew upon my background as a volunteer for a perinatal mental health warm line.
What need does your course fill in the field of pelvic rehabilitation?
Pelvic rehabilitation providers regularly interact with people who have mental health challenges. However, there are very few courses that specifically address the needs of the pelvic health providers serving folks in the perinatal period. This course looks at perinatal mental health from the perspective of pelvic rehabilitation providers, while offering specific actions providers can take to support their clients.
Who, what demographic, would benefit from your course?
Rehabilitation providers of any experience level would benefit from taking this course. Providers who are new parents or considering becoming pregnant may also find the content personally enriching. While the research discussed in this course focused on the perinatal period, much of it can be extrapolated to other populations.
What is your message to course participants who are just starting their journey?
For people just starting in pelvic rehabilitation, I would recommend focusing on patient education. For me, I find that the greatest amount of client improvement comes through reviewing the basics. It’s okay to still be developing skills in manual therapy.

Perinatal Mental Health: The Role of the Pelvic Rehab Therapist
Price: $150
Contact Hours: 5.75
Course Date: October 22, 2022
Description: This one-day remote course covers mental health considerations in pregnancy and postpartum and is targeted to the pelvic rehab clinician treating patients in the peripartum period. Topics include common mental health concerns in the postpartum period including depression, anxiety, OCD, and PTSD, as well as the connectedness between mental health and physical dysfunction. The course will introduce useful screening tools and how to connect patients to resources and diagnosing professionals. Labs will include partnered breakout sessions to practice listening and dialogue skills. The course also includes a review of coping techniques to support mental health and physical symptoms.

This week for the Pelvic Rehab Report, Holly Tanner sat down to interview faculty member Erica Vitek, MOT, OTR, BCB-PMD, PRPC on her specialty course Parkinson Disease and Pelvic Rehabilitation. If you would like to learn more about working with this patient population join Erica on June 24th-25th for the next course date!
This is Holly Tanner with the Herman and Wallace Pelvic Rehab Institute and I'm here with Erica Vitek who's going to tell us about of course that she has created for Herman and Wallace. Erica, will you tell us a little bit about your background?
Yes. Absolutely. Thanks for chatting with me today about my course! So my course is Parkinson Disease and Pelvic Rehabilitation. I'm just so excited to be part of the team and to be sharing all this great information. How I got the idea for the course is that there was a need for more neuro-type topics related to pelvic health, and individuals were reaching out to me because my specialty is in both Parkinson disease, rehabilitation, as well as pelvic health, and I always talked about the connections and wanting to bring that information to more people. So I wanted to plate all that information together in this great course.
I got started specializing in Parkinson's back in the early 2000s. I was hired at a hospital as an occupational therapist working with people with Parkinson disease. But when I was in college my real interest was pelvic health. So I kind of got thrown into learning a whole lot about Parkinson disease at that time and I got really interested in how it all related to what I really wanted to do, which was pelvic health. I was able to connect that all, really right from the beginning of my career. Even though I started more on the physical rehabilitation side of Parkinson disease, which I continue to this day. I am able to combine those two passions of mine.
I also am an instructor with LSVT Global(1)and so we do LSVT BIG®(2) course training and certification workshops and I work with them a lot. I also have still a physical rehab background, as well as my connection to the public health background, and I bring that all together in my course Parkinson Disease and Pelvic Rehabilitation. We have two packed-full days of information and I think really it does translate well to the virtual environment.
What are the connections between neuro and pelvic health? Can you talk about what some of the big cornerstone pieces are that you get to dive into with your class?
The beginning of the course on the first day is going back to the basics of neuro in general. Really getting our neuro brains on and thinking about terminology, topics related to neurotransmitters and the autonomic nervous system. Individuals with Parkinson’s specifically, their motor system is affected but also their non-motor systems. This includes autonomic function, the limbic system, and all of the different motor functions that also affect the pelvic floor in addition to all of the other muscles in the body.
We have all of this interplay of things going on that affect the bladder, bowel, and sexual health systems in individuals with Parkinson's that is a little bit different than your general population. There are a multitude of bladder issues that are very specific to the PD population, for example, overactive bladder.
This is just one example of the depths we go into right in the beginning on day one where we get into the neuroanatomy and neurophysiology of why that is actually happening. This then helps us go into day two where we talk about the practicality of what you do in the clinic about the things that are happening neurologically which is causing all of these bladder, bowel, and sexual health issues.
What kind of tools do you give to people to help practitioners understand and implement a treatment program?
People with PD are on very complex medication regimens and many of them are elderly, so the medication complexity is much more challenging in this population. At the end of day one, the last lecture, we go through the pharmacology very specifically for people with Parkinson’s in order to have a base of understanding of how that is interplaying with the pelvic health conditions.
We set the baseline of getting that information from your patient off the bat, then discuss what you want to be looking for when you start off with that patient and the importance of finding out what kind of bladder and bowel medications they have taken thus far and how that can potentially interplay with their Parkinson’s. Individuals with PD can have potentially worse side effects from some of those medications that are used for bladder issues specifically. We dig into what to look for, we talk a lot about practical behavioral modifications using bladder and bowel diaries and things like that to weed out some things in addition to using our other skills as pelvic health practitioners.
How can people prepare themselves to come to Parkinson Disease and Pelvic Rehabilitation, are there required readings or things that would be helpful for people to catch up a little bit on the pelvic health or neuro side?
I feel like, and I hope, that I did a really good job at the basic review right at the beginning so we can talk through these topics together. I prefer to take a course and not have to spend a lot of extra time on the pre-recordings because sometimes that can be overwhelming with busy lifestyles. When I put together this course I really wanted us to focus together as a group as we start the class to dig into those basics at the beginning and not have a lot of required things to do prior.
So what I did at the beginning of the course is to make a lot of tables, a lot of charts, and a lot of drawings, that we can reference (we don’t have to memorize it) and look at as needed. We can look at a chart and a drawing right next to it in the manual. I spent a lot of time just putting it all down in words, what I’m saying, so you don’t have to take a lot of notes. I think this has really helped practitioners as we get into the course and learn about the details of Parkinson’s and pelvic health.
What is it that makes you so passionate about working with these patients and continuing to learn and share your knowledge?
It is so heartwarming and feels so good to help these individuals. The motor symptoms of PD are really the ones recognized by physicians or even outwardly noticed even by other individuals. These private conditions of pelvic health that we are helping with are things that they might not even mention to their physician. Maybe we find out when we are doing other physical rehab or when colleagues refer them to us because they know what we do, and to help them with something of this magnitude that affects their everyday life - when they have trouble just walking, or moving or transferring.
Their caregiver burden for these individuals is so high because their loved one - now turned caregiver - is helping them do everything. We can make such an impact on these individuals. I mean, we do on other people too, but when you have a progressive neurologic condition and we can make an effect on shaping techniques they can use to improve their day-to-day. It’s just so great to be able to help them.
Sometimes these patients with PD can have cognitive impairments, they can have difficulties learning, and that can be helpful for the care partner. It can be a significant reduction in their burdon. I do talk a lot in the course about cognitive impairment and I give a lot of tips about how we can train and some ideas. People with Parkinson’s muscles and minds are a little different so there are some great tips that I can provide and lots of clinical experience.
I’ve been an occupational therapist for over 20 years, so I have a ton of clinical experience with this population. It’s been the population I’ve worked with my entire career. I hope I can provide the passion that I have for working with these individuals as well as the individuals who take my class.
I’m sure you would agree that we need more folks knowledgeable about Parkinson’s and combine that with pelvic health knowledge as well.
There are over a million people in the United States alone that have Parkinson disease. It’s the second most common neuro-degenerative disorder just behind Alzheimer’s disease. So there are so many individuals dealing with this and I think we can really expand our practices. I don’t think a lot of individuals that work in pelvic health market themselves to neurologists. There is an opening there for additional referrals and more people that we can help.

References:
- SVT Global is an organization that develops innovative treatments that improve the speech and movement of people with Parkinson’s disease and other neurological conditions. They train speech, physical and occupational therapists around the world in these treatments so that they can positively impact the lives of their patients.
- LSVT BIG®: Physical Therapy for Parkinson’s Disease and Similar Conditions. LSVT BIG trains people with Parkinson disease to use their body more normally.


The following is an excerpt from the short interview between Holly Tanner and Tara Sullivan discussing her course Sexual Medicine in Pelvic Rehab. Watch the full video on the Herman & Wallace YouTube Channel.
Hi Tara, can you introduce yourself and tell us a little bit about your background?
Sure! So I’m Tara. I’ve been a pelvic health rehab therapist for about 10 years now. I started right out of PT school and I got a job at a local hospital where they were looking to grow and build the pelvic rehab program. So of course, I found Herman & Wallace and started taking all of the classes there that I could and just kept learning over the years. Now the program is expanded across the valley, we have nine different locations, and it’s been very successful and fulfilling. It’s my passion.
Recently, I would say the past four to five years of my career, I’ve started getting more into sexual dysfunctions. I was always into pelvic floor dysfunction in general - bowel, bladder, sexual dysfunction, and chronic pelvic pain, but I didn’t get specifically into the sexual medicine side of it until recently. I did the fellowship with ISSWSH that really pulled all of that information together with what I’ve learned through the years.
Can you explain what ISSWSH is and how that combined with the knowledge base that you already had?
I feel like ISSWSH for me, where I came full circle. I finally was like “I get it.” ISSWSH is the International Society for the Study of Women’s Sexual Health and it’s all the gurus like Dr. Goldstein, Rachel Rubin, and Susan Kellogg that have been around forever doing the research on sexual medicine. I started attending their conferences, became a faculty member, and presented at their annual fall meeting here in Scottsdale. Then I ended up doing their fellowship. Every year I would attend the conference, but it took a couple of years for all of that knowledge to soak in and for me to be able to really apply it. For example, that patient with that sticky discharge, maybe that is lichen planus – that’s the kind of medical side that you don’t necessarily learn in physical therapy school.
That for me just really helped my differential diagnosis which means that you can get the patient’s care faster. Get them to that resolution faster because you are working with a team of people and we all have our roles. As PTs and rehab practitioners, we have the time to sit with our patients. We are so blessed to have an hour, and the medical doctors don’t, for us to really take that time to figure out the patient’s history and what they’ve been through, and what could be the cause of it. We have the time to be the detective and help them get the care they need. Whether it’s with us, or in conjunction with something else. My goal is to never tell someone that I can’t help them because it’s not muscular.
How has this knowledge helped you in your collaboration with other practitioners in your practice?
I feel like this knowledge was the missing link for me. It brings it all together for the patient. So the patients come here and the urologist says “that’s not my area,” and then the gynecologist says “that’s not my area.” Then they come to you and you’re like “it’s kind of my area, but I can’t prescribe the medication that you need.”
My practice got so much better, just in the sense of the overall quality of care, when I was able to develop those relationships with the doctors. I could pick up the phone and say “Hey, that patient that you sent me – I think they have vestibulodynia, and I think it’s from their long-term use of oral contraceptive pills. I think that they might benefit from some local estrogen testosterone cream.” They would say, I don’t know about that, and I’d respond “let me send you some articles. Let me tell you what I’ve learned.”
Now I can just pick up the phone or send them a text asking them to prescribe so and so. It really helped bridge that gap. The doctors now will say “Ok. I know something’s going on, but I don’t know if it’s muscular or tissue. I don’t have that training, what do you think?” So it’s just been such a collaboration, it’s been so great. Then I’ll go the reverse of that and watch them do a surgery, watch them do a procedure.
For our patients, we need to take that time and work with the physicians and develop that relationship with them, because it’s easy to pass it off as “that’s not my job.” Especially the vestibule! The gynecologist goes right through it and looks into the vaginal canal and then the urologist is like I’m going to look at the urethra but I’m not looking around it, let me just stick that scope in. This knowledge and ability to use differential diagnosis, for me just brings it all together.
Does your course have an online, pre-recorded portion as well as a live component?
Yes. There are about nine lab videos on manual techniques because everyone wants to know what to do. For me, it’s more about what you know. What can you identify and differentiate with the differential diagnosis. Then we have about two hours of just the basic lectures on general pain and overactivity of the pelvic floor so that we can spend our time in the live lecture getting into the very specific conditions that we as PTs are, not necessarily diagnosing, but recognizing and sending for further care. That’s really where I wanted this class to fill the gap between the urologist, the gynecologist, and the PT.
Is your course primarily vulvo-vaginal conditions or are there some penile, scrotal, or other conditions?
It is both male and female dysfunctions, and I have a few transgender cases. I don’t personally treat the transgender population very often so I only have a couple of examples of that. I have a lot of examples where I’m trying to get practitioners to recognize the problem by what the patient is saying and their history, and how to funnel this into their differential diagnosis. Case studies include different types of vestibulodynia and causes, all the different skin conditions…and it’s not necessarily something that they didn’t learn in one of the Pelvic Floor Series courses, but I wanted one class where they could just talk about all the sexual dysfunctions and get into some of the ones that we don’t see as often but are present.
We also talk about PGAD (persistent genital arousal disorder), and with male dysfunctions, we talk about spontaneous ejaculation and urethral discharge, post vasectomy syndrome. All of these things that you might not see every day, but when you see them you’ll recognize them so that you can help patients talk to the doctor and get the proper care. There are a lot of random, not as obvious, conditions that are not as prevalent. Then there are the common conditions that we see every single day like lichens.
What is the biggest takeaway that practitioners have who come into your class?
It is really being able to access and effectively use differential diagnosis. A lot of practitioners in the course are like “I always wondered what that was.” I have a ton of pictures that I share, and I’m like, I know you guys have seen this before. I think a lot of it is the differential diagnosis. The feedback that I get from every class is “I feel like I can go to the clinic on Monday and apply what I learned.” “I’m going to go buy a q-tip and start doing a q-tip test because now I know what to do with that information.” They feel that confidence of really being able to apply it, talk to the patient, talk to the doctors, and figure out that meaningfulness.

2022 Course Dates:
July 16-17 2022 and October 15-16 2022
Sexual Medicine in Pelvic Rehab is designed for pelvic rehab specialists who want to expand their knowledge, experience, and treatment in sexual health and dysfunction. This course provides a thorough introduction to pelvic floor sexual function, dysfunction, and treatment interventions for all people and sexual orientations, as well as an evidence-based perspective on the value of physical therapy interventions for patients with chronic pelvic pain related to sexual conditions, disorders, as well as multiple approaches for the treatment of sexual dysfunction including understanding medical diagnosis and management.
Lecture topics include hymen myths, female squirting, G-spot, prostate gland, female and male sexual response cycles, hormone influence on sexual function, anatomy and physiology of pelvic floor muscles in sexual arousal, orgasm, and function and specific dysfunction treated by physical therapy in detail including vaginismus, dyspareunia, erectile dysfunction, hard flaccid, prostatitis, post-prostatectomy, as well as recognizing medical conditions such as persistent genital arousal disorder (PGAD), hypoactive sexual desire disorder (HSDD) and dermatological conditions such as lichen sclerosis and lichen planus. Upon completion of the course, participants will be able to confidently treat sexual dysfunction related to the pelvic floor as well as refer to medical providers as needed and instruct patients in the proper application of self-treatment and diet/lifestyle modifications.
Audience:
This continuing education course is appropriate for physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals of all levels and experience. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.


Herman & Wallace is committed to providing courses on pelvic rehabilitation for all people across the spectrum. This week the featured courses are those focused on women's health!
Take a look and see if there is one that is a good fit for you.
Breastfeeding Conditions Remote Course - Remote Course
July 16 and November 19
This course provides a thorough introduction to the physiology of the lactating breast, dysfunction and treatment interventions, the therapist's role in breastfeeding and pumping support, as well as when to refer to other health professionals.
Lectures will include the anatomy and physiology of lactation, blocked ducts and mastitis, and breast pain through a biopsychosocial lens. During labs, participants will have the opportunity to systematically assess the breast and practice therapeutic breast massage and manual milk expression. Participants will learn to assess and treat breast inflammation and pain such as mastitis, blocked ducts, milk blebs, and cracked nipples.
Breastfeeding Conditions - July 16-17, 2022
Breastfeeding Conditions - November 19-20, 2022
Menstruation and Pelvic Health - Remote Course
July 16-17, 2022

Menstruation and Pelvic Health is a two-day remote course is designed for clinicians who want to obtain advanced knowledge and skills to educate patients on non-hormonal, non-surgical, and non-prescription interventions for improving the Menstrual Experience. Developed by Nicholas Gaffga, MD, MPH, FAAFP, and presented together with Amy Meehan, PT, DPT, MTC, this course is geared toward the pelvic rehab provider looking to impart Menstrual Interventions that:
- Put control in the hands of people who menstruate to identify and carry out the interventions that are appropriate to them
- Use a holistic approach and advanced knowledge and familiarity with body and mind
- Emphasize healthy practices that can positively impact the Menstrual Experience and beyond, in areas such as mental health and chronic diseases
- Discover root causes of issues, rather than quick fixes, to have benefits that are sustainable across the lifespan.
Postpartum Rehabilitation - Remote Course
offered monthly through November

The client who is postpartum may be one of the most overlooked clients in health care. Knowing the specific rehabilitation needs to help with common problems and prevent future problems is the goal of this beginner-level course. For the orthopedic-based practitioner, this course will solidify awareness of the common orthopedic needs of the postpartum client. For the non-orthopedic practitioner, this course will provide a foundation for working with clients experiencing common postpartum-related musculoskeletal conditions.
This course will cover examination considerations and modifications specific to postpartum, as well as specific questions to ask during history taking and methods for identifying red flags in postpartum. More comfortable positions during the examination/treatment and common posture/gait/balance changes during postpartum are covered. The participant in this course will understand necessary biomechanics training for daily activities, child care, and breastfeeding. As an expansion from the pregnancy rehabilitation course, participants will be taken through progression in diastasis rectus abdominis (DRA) assessment and rehabilitation, including DRA exercises in lecture and lab.
Postpartum Rehabilitation - July 23-24, 2022
Postpartum Rehabilitation - August 20-21, 2022
Doula Services and Pelvic Rehab Therapy - Remote Course
August 6 and December 10
A growing number of pelvic health therapists are recognizing the importance of preparing their clients for the physical and mental challenges of labor and delivery. In some cases, this is extending to a desire to be present during labor for support as a Doula. The purpose of this course is to present the unique challenges of merging a rehab practice with Doula services in order to help the participant better discern whether or not this is a journey worth taking.
Doula Services and Pelvic Rehab Therapy - August 6, 2022
Doula Services and Pelvic Rehab Therapy - December 10, 2022
Fertility Considerations for the Pelvic Therapist - Remote Course
August 13

This course is for practicing pelvic rehabilitation therapists and covers the role of rehabilitation therapists in optimizing female fertility. This course was written and will be instructed by Dr. Yeni Abraham, who is a Dallas-Ft.Worth-based Pelvic Physical Therapists specializing in the treatment of Gynecologic and Fertility related conditions. Lecture topics include medical infertility labs, pertinent information on charting cycles, assisted reproductive technologies and their impact on treatment, hormone regulation, the relationship between inflammation and infertility, amongst other topics. Lab activities/break-out sessions will include manual techniques to influence uterine and ovarian Mal-positions.
*This course will require that each student have a live model that will allow participants to practice the lab techniques on a human body. Due to the nature of labs, please be sure your model partner is not pregnant and does not have an IUD for safety. Additionally, those with hydrosalpinx will not be able to participate in uterine mobility techniques but can still attend the course.
Fertility Considerations for the Pelvic Therapist - August 13, 2022
Menopause Transitions and Pelvic Rehab - Remote Course
August 27-28th and November 12-13th

Menopause Transitions and Pelvic Rehab is a two-day course is designed for the clinician that wants to understand the multitude of changes that are experienced in the menopause transition and how they affect the aging process. Upon completion of this course, participants will have a basic understanding of the hormonal changes during menopause, the impact on various health systems, and interventions that can assist with improving this transition.
This is an excellent opportunity to understand the physiological consequences to the body as hormones decline, in order to assist our patients in lifestyle habits for successful aging. Topics will include cardiovascular changes, metabolic syndrome, bone loss and sarcopenia, neurological changes (headache, brain fog, sleeplessness), Alzheimer’s risk, and urogenital changes. Symptoms and treatment options will also be discussed, including hormone replacement, non-hormonal options, dietary choices, and exercise considerations.
Menopause Transitions and Pelvic Rehab - August 27-28, 2022
Menopause Transitions and Pelvic Rehab - November 12-13, 2022
Medical Perspective in Peripartum Care - Remote Course
September 17-18th

Medical Perspective in Peripartum Care is a two-day course instructed by Dina Gordon, MD, FACOG, a practicing OB/GYN in the Seattle area, and will discuss common conditions encountered in the peripartum period from the medical perspective. Topics include medical screening; medical management of high-risk patients (bed rest, activity limitations, medications, surveillance); and interventions common in the peripartum period
The course is built from the medical perspective, the design of the course aims to share knowledge so that rehabilitation care planning is optimized.
Medical Perspective in Peripartum Care - September 17-18 2022
Pregnancy and Postpartum Considerations for High Intensity Athletics
September 11

The main focus of this course will be to learn how exercising throughout pregnancy, or returning to exercise postpartum may look different for a high-intensity athlete versus a non-HIIT athlete. Participants will discuss how anatomical and hormonal changes affect training for the pregnant and postpartum athlete, review various modifications for this population, learn how various stresses placed on the body during these activities may affect pelvic floor muscle function, and review various pressure management strategies that can be utilized during high-intensity interval training. This one-day remote continuing education course is designed to educate practitioners on the unique considerations of pregnant and postpartum athletes engaging in high-intensity interval training (HIIT).
During the pregnancy lab, we will review specific exercise modifications for pregnancy, utilization of breathwork to properly support the pelvic floor during pregnancy and review how to assess for and tape for diastasis recti. In the postpartum lab, we will review how to determine proper activity modification based on the ability to manage pressure, review specific activity modifications and breathwork, review accessory work for return to activity, and discuss how to assess pelvic organ prolapse in standing.
Pregnancy and Postpartum Considerations for High Intensity Athletics - September 11, 2022
Perinatal Mental Health: The Role of the Pelvic Rehab Therapist
October 22
This one-day continuing education course covers mental health considerations during pregnancy and postpartum and is targeted to the pelvic rehab clinician treating patients in the peripartum period. Topics include common mental health concerns in the postpartum period including depression, anxiety, OCD, and PTSD, as well as the connectedness between mental health and physical dysfunction.
The course will introduce useful screening tools and how to connect patients to resources and diagnosing professionals. Labs will include partnered breakout sessions to practice listening and dialogue skills. The course also includes a review of coping techniques to support mental health and physical symptoms.
Perinatal Mental Health: The Role of the Pelvic Rehab Therapist - October 22, 2022
Pregnancy Rehabilitation - Remote Course
October 29-30 and November 5-6

Learn how to safely examine and treat the pregnant patient in this beginner-to-intermediate course.
Lectures cover terminology, fertilization, trimesters, medical testing/interventions, imaging, and medications. Participants will learn to differentiate between false labor, progressive labor, and other musculoskeletal pain as well as learn to understand typical hormonal and systemic changes during pregnancy. Examination, evaluation, and treatment of common lumbopelvic conditions will be provided with an introduction to diastasis rectus abdominis, pelvic floor dysfunction, breathing, and deep core assessment/treatment.
Discussions also include general examination considerations and modifications specific to pregnancy, including a discussion of modalities and manual therapy techniques considered safe or precautioned during pregnancy, with further lectures on pelvic girdle examination, diagnosis, and treatment strategies. Finally, to prepare the pregnant client for labor and birth, instruction in perineal stretching, hip and trunk flexibility activities and TENS for labor will be discussed. Lab practice will include labor and birthing positions, with a focus on consideration for positional strategies for women with pre-existing musculoskeletal problems.
Pregnancy Rehabilitation - October 29-30, 2022
Pregnancy Rehabilitation - November 5-6, 2022
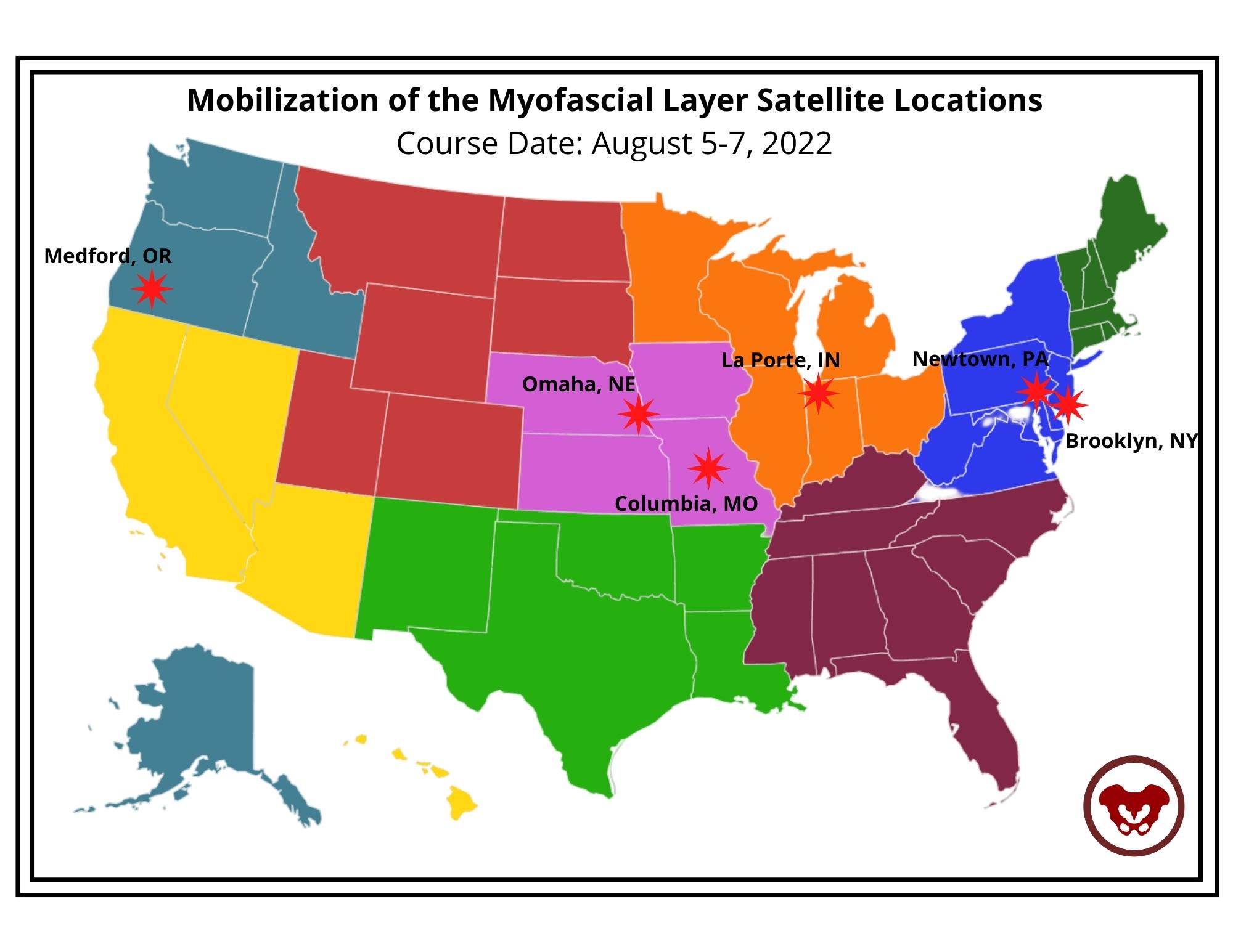
This week Ramona Horton sat down with Holly Tanner to discuss manual therapy and her course Mobilization of the Myofascial Layer: Pelvis and Lower Extremity. The following is an excerpt from her interview.
What do we really know about manual therapy? We have decent evidence that shows that asymmetry matters. The tenet of the myofascial course is an osteopathic tenet called ARTS:
- Asymmetry
- Restriction of Mobility
- Tissue Texture Changes
- Sensitivity
The whole myofascial course is designed around looking for ARTS. When you find the asymmetry within the myofascial system then that’s where you direct your efforts and energy.
Often patients have already tried breathing, yoga, medication, etcetera – and it’s the manual therapy piece that they often have not had. It’s not that uncommon for me to be someone’s second or third therapist. Some patients may have tried some type of manual therapy but it was more things like ischemic compression where the problem was that the manual therapy was triggering nociception.
So in the myofascial course, we start with ARTS but we also have an idea where we flip ARTS on its head and we go to STAR. In STAR, you take sensitivity and put it at the top of your list. That becomes the highest portion in your paradigm. Then we use simple techniques that are not non-nociceptive. Indirect technique versus direct technique, such as something as simple as positional inhibition.
The whole idea of the myofascial course is to teach people to think and problem solve. Then have a very broad spectrum way of you find an inner articular issue where this joint is moving and this one is not. Learn to not chase the booboo. Just because it hurts on the right doesn’t mean that you’re going to treat the right. It might hurt on the right because there is a hypo-mobility on the left. Let’s treat where the brain is protecting the tissue, and holding, and guarding the tissue. Trust in the belief that the body is a self-righting mechanism. The body will then normalize itself.
In manual therapy, our job is to get the body moving like it's supposed to. It’s not to fix the ‘booboo.’ The issue is not in the tissue. If the tissue is tight, it’s tight because the brain is keeping it that way. The way I teach manual therapy is the fascial system gives us access to the nervous system. By utilizing the fascial system in a non-nociceptive manner, what we’re really doing is just having a conversation with the brain. We’re not fixing the tissue. That’s the whole premise of the course - to get people to understand and change their thinking and their paradigm to ask what the brain is protecting and utilizing the fascial system.

Course Date: August 5-7, 2022
- Self-Hosted - for groups of at least 2 qualified practitioners.

Congratulations to Dr. Mia Fine (they/she) for achieving their Ph.D. in Clinical Sexology and on their book titled 'From Unwanted Pain to Sexual Pleasure: Clinical Strategies for Inclusive Care for Patients with Pelvic Floor Pain' for their dissertation doctoral project.
Dr. Fine was gracious enough to share a draft of their dissertation with Herman & Wallace and to answer a couple of questions about how this impacts their practice and what they hope other practitioners will take away from their book and course Sexual Interviewing for Pelvic Health Therapists.
Mia's course is for the pelvic rehab therapist and others in the medical profession who work with patients experiencing pelvic pain, pelvic floor hypertonicity, and other pelvic floor concerns and would like to learn applicable skills from the sex therapist's clinical toolkit. The next course date for Sexual Interviewing for Pelvic Health Therapists is August 13-14,

How does Trauma-Informed Care apply to the skills that you teach in your Sexual Interviewing course?
When I utilize the term ‘trauma-informed’ I am referring to therapeutic work that communicates expectations clearly (including prioritizing people’s access needs with this communication), invites clients awareness of their own agency, and is upfront about my scope of practice and my therapeutic approach, offers mutuality in inviting of questions and ongoing conversation about our work together, awareness that an individual can end therapy at any time, and share information at any time in our therapeutic space.
The modalities I utilize when working with clients who have experienced trauma include Eye Movement Desensitization and Reprocessing (EMDR), Polyvagal Theory, Somatics, and Developmental Theory. While I integrate various theories and modalities into my work with clients, the methods above are empirical in their data to support healing from trauma wounds.
Trauma-informed means humility regarding cultural, racial, gender, sexual, and other minority experiences. I will not know all of the things but I will do my best to self-educate and not leave that responsibility to my clients. When I make a mistake I will appropriately, directly, and compassionately apologize for the harm I caused and invite opportunity for repair should the client be interested. Trauma-informed means collaboration in exploring therapy together, co-creating a space that feels safer to the client and checking in with them when I notice non-verbal cues that indicate activation, honoring a client’s pacing, and bringing awareness to the reality that as a therapist I hold power and while I don’t know a person’s full story there is always the potential for me to unintentionally activate a client so to share this possibility with clients and continuously check in about how our therapy is working for them. I keep my client’s well-being at the forefront of our work and I center their needs at all times while maintaining boundaries that keep everyone as safe and secure as possible.
It is up to us as trauma-informed and inclusive providers to explore a person’s experience of pain by asking questions about onset, process, location, and impact, in addition to offering psychoeducation about anatomy, physiology (arousal, interest, desire), and self-regulation. This must be done alongside commitment to our patient’s co-regulation, normalization, and informed consent concerning the therapeutic process—all of which are needed for comprehensive trauma-informed care.
Can you explain how expanding what 'normal' is to practitioners can impact the patients and clients that they work with?
Sex is not supposed to be painful. How many people have come to me having had painful sexual intercourse for years and reported “pushing through”? The first time having intercourse does not necessarily have to be painful, but when our cultural narratives tell us “the first time having sex is painful for everyone” we end up ignoring the signals our bodies are offering because we have convinced ourselves that the pain is both okay and normal. The “pushing through” is a reflection of misogyny: people assume the first experiences people have with penetration are supposed to be painful. How is this misogynistic? Well, who benefits from a person “pushing through” pain? The partner with the penis. Important to note here as well is that enthusiastic consent is ableist and ignores the mind-body connection because it does not take into account masking or fawning which are common experiences for many.
A quarter of people who experience sexual health concerns share this with their providers. Why such a small fraction? Fear. Fear of embarrassment and shame. Fear that there is something “abnormal” about them that mutates into the shame humans tend to experience in response. Fear that the concern won’t be held or taken seriously by their provider. Fear that, if it is addressed, will be at such a high financial cost that the treatment will be unaffordable. Fear that there’s not enough time or that they won’t be taken seriously. Fear of exclusivity, feeling othered, or misunderstood by their provider. Fear of the unknown because the reality is that people are afraid of what we don’t understand.
One of the major cultural issues we have in the US is the perpetuation of sexual stigma which is largely associated with a lack of comprehensive sex education. People don’t have access to basic information about their own bodies which influences our beliefs about sex, pleasure, agency, communication, and self-awareness. Sex education should be a birthright, and yet we are so far behind the curve that it sometimes feels impossible to break down the barriers.
When I first started in this career it would often take clients months of working with me to feel comfortable enough to talk about where they felt pain during sex, but in developing the tools to co-create safety in our therapeutic relationship and the skills to ask the important questions with compassion and patience, I learned how to better hold space for healing.
Patients don’t often know what information is important for them to share with us (which is why offering visuals of where the pain is located is important). How could they know what information is important to offer when mental and sexual health are so deeply stigmatized? The stress of shame and embarrassment that people feel about their bodies is emotional pain that further exacerbates the physical pain that they came to therapy to address in the first place. It’s a terrible and self-perpetuating cycle.
I teach people the difference between a vulva and a vagina one thousand times a year. If a client does not know the terminology for labia, vulva, vagina, and clitoris, how are they supposed to know when their sexual health is of concern? If a person enters sex therapy with “sexual pain” but is unable to distinguish the difference between their labia and vagina (that they are different body parts, where they are located, and what their functions are) we cannot expect them to accurately articulate the location of pain or comprehend potential solutions. “What is your hygiene process when cleaning your vulva?” may activate the fight or flight response in clients if they do not know what their vulva is or that there could be a good hygiene process, in addition to the shame of not knowing. How are they supposed to know where or to whom they may ask for help?
An online search for “anatomical vulva”, “pelvic floor pain”, “vaginismus treatment” and 99% of the images and figures you will see are those of hairless, slender bodies with white/light skin and small labia. Racism and white supremacy are present everywhere. The anatomical depictions of vulvas are of white bodies, the people modeling in vaginismus treatment advertisements are white, and the language is geared toward and written for white people. I was intentional about not featuring white vulvas in this book because white bodies should not be the default of what is mainstream. This lack of diversity in skin tone and variation of body type is another reflection of racism called “colorism”. White and light skin bodies are viewed as more ‘normal’ and when we continue to center white bodies in visuals “because that is what is available” we perpetuate white supremacy. One goal is to disrupt the idea and practice of whiteness as the default. This is what it means to practice anti-racism and attempt to divorce ourselves from white supremacy.
The impact of shame shows up in the pervasive erotophobia rampant in our society. Erotophobia can be broadly defined as a “fear of sex” or more specifically a “fear of intercourse”. When erotophobia is judgment as a result of societal shame and stigma, we can navigate it by deconstructing the etiology and impact of messages received; when it is a result of a mental health condition such as Obsessive Compulsive Disorder (OCD) or Post Traumatic Stress Disorder (PTSD), we do deep trauma and/or anxiety/exposure work. Because of the vast impact of shame, people fear sharing sensitive information about themselves with others, including therapists who are trained to help them. Often, therapists are untrained in sexual health which also can contribute to erotophobia and shame. When therapists have not done their own work on sexuality, and remain untrained in these areas, they may be afraid to discuss sex with their clients which reinforces the belief that topics regarding sex are shameful.
When people do not have the language to articulate what is happening in their body, as significant as the pain or discomfort might be, talking about sex with a provider is often the last item on a long list of concerns they bring to a medical appointment. Symptoms of sexual pain may be hidden by other “more pressing” concerns such as anxiety, depression, PTSD, or sleep issues. While these are of course vital for a medical provider to know, having 20 minute appointments with a physician who will prioritize the “presenting concern” that they came in to seek treatment for leaves very little time to discuss unwanted sexual pain. After 15-20 minutes of a medical appointment (if it goes well), a patient might feel comfortable enough to bring up their sexual concern, but this might leave 1 minute for it to be acknowledged and no time to conduct a comprehensive assessment or develop an intentional plan. We call these last-minute oh-by-the-way’s “door-knobbing” for a reason. This is a call for medical clinics to have training in sexual health so they can create intake documentation that explores clients’ sexual health and ask the questions that are vital to gather necessary information ahead of time.
In the same way that people lack language and anatomic understanding, people also lack awareness of the mind-body relationship. Due to the ableist sex-negative culture in which we live, people are often not taught to have knowledge of or listen to our own body. We’re not taught that pain is a signal from the body telling us that something’s wrong.


Instructor Sarah Hughes, PT, DPT, OCS, CF - L2 sat down with The Pelvic Rehab Report to answer a couple of questions about treating the Crossfit and weightlifting community. Dr. Hughes earned a BS in exercise science from Gonzaga University and a DPT from the University of Washington.
Sarah's specialties include dance medicine, the CrossFit and weightlifting athlete, and conditions of the hip and pelvis such as femoroacetabular impingement and labral tears. She began coaching other PTs who wanted to start their own practices in 2017 and co-founded Full Draw Consulting with her partner Dr. Kate Blankshain.
Sarah teaches Weightlifting and Functional Fitness Athletes, which s scheduled for August 7th and October 15th of this year.
What are three things you wish you knew when you first started treating the athletic community?
First, I wish that I had had the confidence to treat these athletes the way I saw fit earlier in my career. For a long time, I felt weird treating CrossFit athletes in the clinics I worked in because I felt that my peers were judging me. My colleagues (and many PTs at the time) were wary about the sport and believed it was dangerous for patients. This is a viewpoint I am working to change in our profession.
Secondly, I wish I knew more about how to scale movements in a way that is relevant to the patients and the stimulus they are striving for. For example, if a patient wants to be able to do kipping pull-ups in a workout, giving them banded strict pull-ups as a substitute is not the only option. What about the metabolic conditioning part of the equation? What about looking at the volume and how that is impacting the tissue of concern? This is a big topic that we discuss in my course.
And finally, I wish I knew that being an effective therapist for these athletes does not mean being the top athlete in the gym. In fact, just as with coaching, you do not have to be a great athlete to be a great PT. Again, this is something that I want to change as far too few physical therapists are comfortable treating these or advertising that they treat these athletes because they are not Crossfit athletes (or are not ELITE Crossfit athletes) themselves.
What lesson have you learned in a course, from an instructor, or from a colleague or mentor that has stayed with you?
One important lesson that has stayed with me came from a colleague in Seattle who started her business a year before I started mine. She told me that I needed to listen to my gut when it came to treating these athletes. She reminded me that my experience with CrossFit as a sport, as an athlete, as a coach, and as a PT put me in a position to be an expert on how to help these folks. What I did not need was to allow other physical therapists to sway my thinking and cause me to doubt myself by insisting that we should not be condoning the sport. TRUST YOUR GUT. If you think you are doing what is right for the patients, you are. You might not be right for every patient and that is OK! I am certainly not the right therapist for everyone, but I am indeed right for the community I serve.
Weightlifting and Functional Fitness Athletes - Remote Course

When it comes to Crossfit and Weightlifting, opinions are divided among Physical Therapists and other clinicians. In this half-day, remote continuing education course, instructor Sarah Haran PT, DPT, OCS, CF-L2 looks at the realities and myths related to Crossfit and high-level weight-lifting with the goal of answering “how can we meet these athletes where they are in order to keep them healthy, happy and performing in the sport they love?"
This course reviews the history and style of Crossfit exercise and Weightlifting, as well as examines the role that therapists must play for these athletes. Labs will introduce and practice the movements of Crossfit and Weightlifting, discussing the points of performance for each movement. Practitioners will learn how to speak the language of the athlete and will experience what the movement feels like so that they may help their client to break it down into its components for a sport-specific rehab progression.
The goal of this course is to provide a realistic breakdown of what these athletes are doing on a daily basis and to help remove the stigma that this type of exercise is bad for our patients. It will be important to examine the holes in training for these athletes as well as where we are lacking as therapists in our ability to help these individuals. We will also discuss mindset and cultural issues such as the use of exercise gear (i.e. straps or a weightlifting belt), body image, and the concept of "lifestyle fitness". Finally, we will discuss marketing our practices to these patients.
Course Dates: August 7th and October 15


Faculty member Ginger Garner PT, DPT, ATC/L is offering a new short course, The Voice and The Pelvic Floor. This course introduces foundational concepts needed to be able to use vocal techniques to treat the pelvic floor and core. Dr. Garner is a clinician, educator, and longtime advocate committed to making physical therapy services accessible, affordable, and equitable, especially for pelvic health.

When you think of pelvic health, what comes to mind? Obvious variables like the pelvic floor & girdle, abdominals and related synergists, mental health, and gut and respiratory health are probably at the top of your list.
But how often do we consider the voice as a biomarker of pelvic health? It can impact all of the variables above and more.
Historically, speech-language pathologists’ study of vocal health has stopped at the respiratory diaphragm, while physical and occupational therapists’ study of pelvic health has stopped, well, in the same place. Neither has traveled beyond that until recently.
However, there is a third diaphragm beyond the respiratory and pelvic, the laryngeal diaphragm. It’s also known as the cervical, cervico-thoracic, vocal, and/or thoracic diaphragm. The three diaphragms include:
- The Laryngeal Diaphragm - is responsible for neurological optimization of stress response and physiological control of swallowing and communication; but, it also influences vagal tone for cardiorespiratory functioning and respiratory and pelvic diaphragm functioning. It contains the muscles that are responsible for phonation, which includes intrinsic variables such as the arytenoids, but also extrinsic components which have a direct impact on the vocal fold health, such as the suprahyoid muscles.
- The Respiratory Diaphragm - is the connecting point between cephalad and caudad diaphragms and is the main muscle influencing pulmonary function. However, the respiratory diaphragm exacts a major influence on mind-body health, which goes far beyond pressure regulation of the vocal and pelvic diaphragms.
- The Pelvic Diaphragm - is the terminal end of the tri-diaphragmatic (3D) system, and can bear the brunt of trauma and impairment if dysfunction is present in the two upstream diaphragms. The pelvic diaphragm contains the levator ani, coccygeus, and related synergists, pelvic fascia, and neurovascular structures, which in turn can work with or against breathing and voicing tasks.
The diaphragms are in constant movement and none work in isolation. Together, their intersectional action provides us with the key to both internal and external biopsychosocial stability and structure of the mind-body.
The laryngeal diaphragm has a supradiaphragmatic vagal impact, while the pelvic diaphragm exacts subdiaphragmatic vagal health, chiefly through afferent and efferent input, respectively. The 10th cranial nerve lives up to its namesake, “the wandering,” as it touches each of the three diaphragms on its journey, harnessing the capacity to lessen pelvic and visceral pain, while also improving vocal quality and lung function, and changing pain, mood, and digestive function.
The mind-body interface of the 3D system has been further defined in recent years, broken down into a voluntary motor system (the one we spend all our time studying and treating), and the “emotional motor system,” and the implications are profound. Anatomists and researchers tell us that in order to generate speech, we need both motor systems to function. But specifically, our emotional motor system must first perceive safety before speech can be produced or produced well.
To get a feel for your own emotional motor system health, try this brief exercise:
- Think about a recent incident that made you feel nervous, or anxious.
- How well could you breathe?
- Talk?
- Sing or hum?
- Engage in intimacy with someone?
Not very well, right? This feeling is the fallout from your emotional motor system perceiving danger or threat. It’s what Dr. Stephen Porges means by the phrase, “neuroception.” Neuroception is the ability to detect risk - but it’s not just the ability to detect it - neuroception is the ability to accurately detect risk.
Here lies the problem:
If we cannot detect external risk or internal threat accurately, aka if our neuroception wiring is faulty, then we may move to 1 of 4 default modes for behavior: fight, flight, freeze, or fawn. If we are left in this state of reactivity, courtesy of the sympathetic nervous system, then polyvagal theory predicts we will enter into a dissociative state, termed a dorsal vagal response (DVR). The DVR drives self-preservation in severe trauma states, which can preserve life; but it is also to blame for bradycardia and left unchecked, death. Especially now post-COVID, it’s imperative that all therapists understand how to recognize, screen for, and help nurture healthy self-regulatory strategies via trauma-informed care.
We must also learn how to create a therapeutic landscape conducive to healthy neuroception, one that appeals to the “safety switch” of the emotional motor system. Establishing this healthy therapeutic alliance with our patients and clients is critical in pelvic health because the same motor system that controls the creation of sound, dictates everything associated with pelvic health, including micturition, defecation, partuition, stress response, and sexual function.
Understanding the basis of “3D” neurophysiology makes targeting the voice a perfect alternate but necessary pathway for successful comprehensive pelvic health care. The ability to create sound literally determines how we interact with the world around us, and whether or not we can do so with empathy and safety. Additionally, the success of our intervention as pelvic health therapists is also determined by the degree to which we are using a biopsychosocial model, which has long been supported as the most effective and cost-effective way to manage pain and tackle chronic disease and impairment.
What does including the voice look like in pelvic health?
For starters, the first step is evaluating the orofacial and vocal health of the patient or client. Second, and perhaps surprising to some, is the evaluation of the therapist’s own voice as a therapeutic agent. These assessments work to identify red flags that place undue stress through the downstream diaphragms and stress response system. More complex assessment can include lumbopelvic ultrasound imaging as well, which provides a more comprehensive way to individualize therapy prescription.
Assessment is essentially a 4-pronged process - The first two prongs consist of building on existing evaluation skills in respiratory, core, and pelvic floor and girdle assessment. The final two include an assessment of the physiological functioning of the orofacial area and voice and an evaluation of psychosocial determinants which would influence cranial nerve and vocal functioning. The voice is an incredible tool for improving pelvic health outcomes, if we learn how to harness its frequency and power.
Join Dr. Ginger Garner for a virtual short course, The Voice and the Pelvic Floor scheduled for October 1, 2022, to learn more.
Sources
- HOLSTEGE, G., 2016. How the Emotional Motor System Controls the Pelvic Organs. Sexual Medicine Reviews, 4(4), pp. 303-328.
- HOLSTEGE, G. and SUBRAMANIAN, H.H., 2016. Two different motor systems are needed to generate human speech. The Journal of comparative neurology, 524(8), pp. 1558-1577.
- Speer LM, Mushkbar S, Erbele T. Chronic Pelvic Pain in Women. afp. 2016;93(5):380-387.
- Miciak M, Gross DP, Joyce A. A review of the psychotherapeutic “common factors” model and its application in physical therapy: the need to consider general effects in physical therapy practice. Scand J Caring Sci. 2012;26(2):394-403. doi:10.1111/j.1471-6712.2011.00923.x
- Padoa A, McLean L, Morin M, Vandyken C. The Overactive Pelvic Floor (OPF) and Sexual Dysfunction. Part 2: Evaluation and Treatment of Sexual Dysfunction in OPF Patients. Sex Med Rev. 2021;9(1):76-92. doi:10.1016/j.sxmr.2020.04.002
- Wijma AJ, van Wilgen CP, Meeus M, Nijs J. Clinical biopsychosocial physiotherapy assessment of patients with chronic pain: The first step in pain neuroscience education. Physiother Theory Pract. 2016;32(5):368-384. doi:10.1080/09593985.2016.1194651
- Porges SW. The polyvagal perspective. BiolPsychol. 2007;74(2):116-143.

Maricel Briones, DPT, CMTPT, OCS sat down with The Pelvic Rehab Report this week to discuss herself and how she came to TA for Herman & Wallace. You can find Maricel this fall TA'ing Pelvic Floor Level 2B in Virginia Beach, VA.
Hi Maricel, can you share a little bit about yourself and your clinical practice?
Hi, I'm Maricel Briones, DPT, CMTPT, OCS and I've lived in Virginia Beach, VA my whole life. I graduated from Old Dominion University with a Bachelor in Exercise Science and followed that up with a Doctorate of Physical Therapy degree. I am now a Partner, Area Director, and Co-Leader of Pelvic Health with Ivy Rehab and have been a practicing therapist since 2012. I became an Orthopedic Clinical Specialist and Certified Myofascial Trigger Point Specialist for Dry Needling and recently became a Pelvic Health Therapist in 2020. My current clinic opened in December 2021, located in the Town Center area of Virginia Beach, VA. We are in the middle of expanding. We are a mix of outpatient orthopedic and pelvic health for men and women. My whole clinic is trained to support each other with all cases, even with pelvic health, and work together as a team for each patient's visit.
What has your educational journey as a pelvic rehab therapist looked like? Where did you start?
I started in early 2020 with Herman & Wallace (H&W) Pelvic Floor Level 1 in Virginia Beach, VA, then continued and took Pelvic Floor Level 2B towards the summer. It started a little slow because of Covid but it picked up in October 2022 and has been very busy since. In 2021, I continued taking more H&W courses including Pelvic Floor Level 2A, Male Pelvic Floor, and Pelvic Floor Capstone. I continued to host around 5-7 H&W courses to review the material and encourage local ortho therapists to join the pelvic health world. I eventually became a teaching assistant (TA) for H&W and have been loving it ever since. I became a Senior TA earlier this year.
How did you get involved in the pelvic rehabilitation field?
My regional director first asked and brought it to my attention, but I declined. A year later, she further explained the impact we can have for patients with pelvic floor conditions and got me convinced. I gave it a shot in 2020 and realized it was where I should be. It's the most rewarding type of treatment we can provide for a patient. We are helping a hidden population that we did not know exists right in front of us. Helping them with critical functions needed in life, voiding, BM, sex, etc.
What patient population do you find most rewarding in treating and why?
Either the pediatric or geriatric population for urinary incontinence (UI). I enjoy teaching them good bladder habits and how to properly contract their pelvic floor muscles. My first patient was an 80-year-old who had urinary incontinence for 20 years and after 1 week of pelvic therapy, she went from changing her pad around 8 times a day to only 2. I had my first pediatric patient who had seen 4 specialists in 1 year for UI. After 2 weeks of pelvic floor rehab, she went from having 4-6 accidents a day to 1-2 every other day.
If you could get a message out to physical therapists about pelvic rehab what would it be?
Don't be afraid of the "V". A lot of PTs are uninterested and do not realize how much pelvic floor muscle training is similar to orthopedic, either stretch it or strengthen it, and provide a lot of education on habits. Also, it's all about functional movement, so connect the pelvic floor with the upper and lower body for optimal outcomes. I did an internal Ivy Rehab Ted Talk in Florida for our Director's Summit in May 2021, titled "Don't be afraid of the 'V'". What you're nervous of or afraid of, may actually be where you are meant to be or do.
What lesson have you learned in a course, from an instructor, or from a colleague or mentor that has stayed with you?
Continue to learn no matter what, and never settle. My treatment programs and assessments evolve every year because of continued learning and advice from colleagues. Always be open to different approaches and be patient with all complex cases.
What do you find is the most useful resource for your practice?
Facebook groups such as Global Pelvic Physio (run by Michelle Lyons), Pelvic PT Newbies (run by Jessica and Andrew Reale), Pelvic PT Huddle (run by PelvicSanity and Nicole Cozean), and Pelvic Floor Biofeedback (run by Tiffany Ellsworth Lee) have been my go-to for learning about cases, ideas, etc.
What is in store for you in the future as a clinician?
I plan to take the PRPC exam soon for board certification. I am also working with Ivy Rehab to create a year-long Pelvic Health Specialization program.
What has been your favorite Herman & Wallace Course and why?
Pelvic Floor Level 2B, since I learned more in-depth manual therapy for the pelvic floor and it helped nail down the anatomy of the pelvic region. I also love the manual therapy skills that we learned in Capstone.
What lesson have you learned from a Herman & Wallace instructor that has stayed with you?
Lengthen before strengthen!
What do you love about assisting at courses?
It's an information refresher. The more you hear it, the more it sticks. I also love teaching the students the concepts and anatomy that were originally confusing for me.
What is your message to course participants who are just starting their journey?
Continue to take more courses on pelvic floor rehab as there are so many different pelvic health conditions. Take the same concepts you learned about muscle training for any body part and apply them to the pelvic region. Connect the pelvic region to the whole body and focus on actively training it with function. It's not just about motor control of the pelvic floor muscles, it's coordinating it with the abdominals, hips, back, etc. Not all visits are hands-on one-on one-on-one. If you create a robust well-rounded program for them and they will progress quicker than you expect.

Alyson Lowrey, PT, DPT, OCS is the co-instructor for the H&W course Pain Science for the Chronic Pelvic Pain Population - Remote Course alongside Tara Sullivan, PT, DPT, PRPC, WCS, IF. Alyson treats the pelvic floor patient population through an orthopedic approach, working closely with pelvic floor specialists.
Pain neuroscience education (PNE) is the explanation of the neurophysiological changes in the central nervous system in patients with chronic pain. It includes how the nervous system functions and factors that influence its function such as social, psychological, and environmental factors. Pain neuroscience education aims to increase the patient’s knowledge about pain, decrease the threat of pain, and allow the patient to reconceptualize pain from a biopsychosocial perspective.
As a clinician seeing a patient with chronic and complex pain, it can be very daunting trying to determine how much education you should give the patient. Patients are generally very invested in improving their quality of life and therefore invested in learning how to treat their pain. Using techniques such as motivational interviewing is one way to determine if a patient is receptive to new information about pain and how to deliver that information. Education about pain needs to be varied and tailored to each patient based on their prior knowledge and perceptions, learning styles, their language, and their health literacy.
When a patient has an increased understanding of their pain and how their nervous system works, it can change their perspective about their pain by decreasing the threat value of their pain. PNE is the first step in the process of increasing a patient’s pain thresholds during exercise and functional activity. When patients no longer fear their pain as a sign of tissue damage, they can become empowered to re-educate their nervous system and pain processing centers in their brain. As providers, we are able to do this in several ways. We can do this by helping build new coping strategies and thought processes around their pain and dispelling misconceptions about their pain and physical ailments. We can suggest lifestyle and movement modifications that allow for more functional movement that doesn’t increase their pain activation centers. We can also adjust and modify our treatment plan around the patient's needs for success at each session. Consistently being a voice of encouragement, empowerment, and validation is also a very important component of PNE and our treatment as clinicians for our patients with chronic pain.
Pain Science for the Chronic Pelvic Pain Population - Remote Course
Course Date
October 8th-9th
Description
This course provides a thorough introduction to pain science concepts including classifications of pain mechanisms, peripheral pain generators, peripheral sensitization and central sensitization in listed chronic pelvic pain conditions; as well as treatment strategies including therapeutic pain neuroscience education, therapeutic alliance, and the current rehab interventions' influence on central sensitization. The rehab professionals who attend will be provided the understanding and tools needed to identify and treat patients with chronic pelvic pain from a pain science perspective. Lecture topics include the history of pain, pain physiology, central and peripheral sensitization, sensitization in chronic pelvic pain conditions, therapeutic alliance, pain science and trauma-informed care, therapeutic pain neuroscience education, the influence of rehab interventions on the CNS, and specific case examples for sensitization in CPP.
All Upcoming Continuing Education Courses

Pelvic Function Level 2B - Satellite - Seattle WA - April 27 - 28 2024 SOLD OUT
Apr 27 2024 - Apr 28 2024



Pelvic Function Level 2B - Satellite - Cranford NJ - April 27 - 28 2024 - SOLD OUT
Apr 27 2024 - Apr 28 2024

Menopause Transitions and Pelvic Rehab - Remote Course - April 27 - 28 2024
Apr 27 2024 - Apr 28 2024

Nutrition Perspectives for the Pelvic Rehab Therapist - Remote Course - April 27 - 28 2024
Apr 27 2024 - Apr 28 2024


Pelvic Function Level 2B - Satellite - Des Plaines IL - April 27 - 28 2024
Apr 27 2024 - Apr 28 2024



Pelvic Function Level 2B - Satellite - Hilton Head SC - April 27 - 28 2024
Apr 27 2024 - Apr 28 2024












Pelvic Function Level 1 - Satellite - Kankakee IL - May 4 - 5 2024 - SOLD OUT
May 4 2024 - May 5 2024

Pelvic Function Level 1 - Satellite - Ann Arbor MI - May 4 - 5 2024 - SOLD OUT
May 4 2024 - May 5 2024

Pelvic Function Level 2B - Satellite - Fairfax VA - May 11 - 12 2024 SOLD OUT
May 11 2024 - May 12 2024


Trauma Awareness for the Pelvic Therapist - Remote Course - May 11 - 12 2024
May 11 2024 - May 12 2024

Pelvic Function Level 2B - Satellite - East Greenwich RI - May 11 - 12 2024
May 11 2024 - May 12 2024


Sacral Nerve Manual Assessment and Treatment - Remote Course - May 11 - 12 2024
May 11 2024 - May 12 2024


Mobilization of Gastrointestinal Visceral Fascia Satellite Lab Course - Self-Hosted - May 17 - 19 2024
May 17 2024 - May 19 2024

Mobilization of Visceral Fascia: Gastrointestinal Satellite Lab Course - Torrance CA - May 17 - 19 2024
May 17 2024 - May 19 2024

Mobilization of Visceral Fascia: The Gastrointesti System Satellite Lab Course - Bedford NH - May 17 - 19 2024
May 17 2024 - May 19 2024

Mobilization of Visceral Fascia: The Gastrointestinal System - Asheville NC - May 17 - 19 2024
May 17 2024 - May 19 2024

Mobilization of Visceral Fascia: The Gastrointestinal System Satellite Lab Course - Lansing MI - May 17 - 19 2024
May 17 2024 - May 19 2024

Mobilization of Visceral Fascia: The Gastrointestinal System Satellite Lab Course - Scarborough ME - May 17 - 19 2024
May 17 2024 - May 19 2024

Mobilization of Visceral Fascia: Gastrointestinal Satellite Lab Course - Medford OR - May 17 - 19 2024
May 17 2024 - May 19 2024

Pediatrics Level 1 - Treatment of Bowel and Bladder Disorders - Remote Course - May 18 - 19 2024
May 18 2024 - May 19 2024

Pelvic Function Level 1 - Satellite - Phoenix AZ - May 18 - 19 2024 - SOLD OUT
May 18 2024 - May 19 2024

Pelvic Function Level 1 - Satellite - Anaheim CA - May 18 - 19 2024 - SOLD OUT
May 18 2024 - May 19 2024