Post-Vasectomy Syndrome
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI is a faculty member and the Director of Education at Herman & Wallace. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. Along with H&W faculty member Stacey Futterman, she co-authored the Male Pelvic Floor course.
In the US, vasectomy is one of the most common procedures performed, and it is often completed in an outpatient setting with a local anesthetic. Fortunately for most folks, it’s well-tolerated and the advice to rest and ice is enough to allow full recovery. Unfortunately, there are those who don’t recover with ease and are left with chronic pain complications. This is a population that is often left out of the clinical rehabilitation setting, and there is not yet robust literature to catch up with the positive clinical results pelvic rehab providers observe when treating post-vasectomy pain.
The Procedure
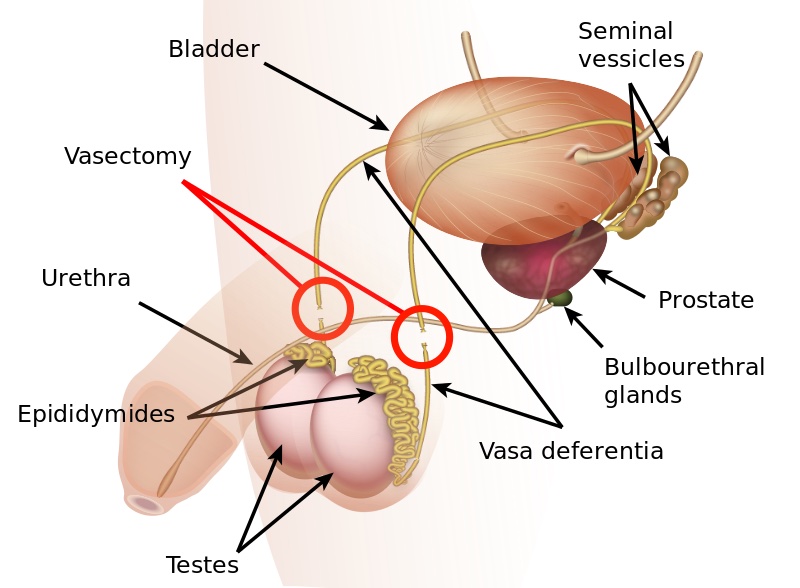
The goal of a vasectomy is typically contraception. The tube known as either the vas deferens or the ductus deferens is interrupted so that sperm does not travel to its typical destination outside the body via the urethra. This disruption in the tube takes place within the spermatic cord as it passes through the scrotum as this area is easily accessible. There are several techniques that can disrupt the tube where the sperm travels including, but not limited to, clamping, cauterization, or excision. The procedure leaves a small incision in the scrotal tissue.
Post-vasectomy Complications
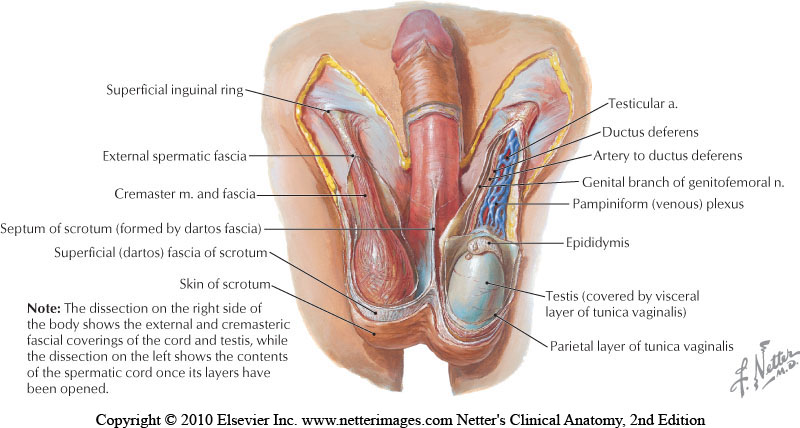
Complications of a vasectomy may include bleeding and hematoma, infection, sperm granuloma (discussed below), chronic scrotal pain, seminal vesicle abscess (rare), and early or late canalization. (Sihra et al., 2007) Interestingly, some patients report less pain after vasectomy. (Leslie et al., 2007) Theories about the cause of post-vasectomy pain include interstitial fibrosis in the epididymal duct and perineurial fibrosis. (Lee et al., 2012) When we consider the anatomy, within the canal there may also be nerve irritation from the genitofemoral nerve, for example, or other connective tissues. If a patient had pain prior to the procedure in the low back, lower abdomen, or groin, the patient’s system may have been vulnerable to complications due to a sensitized system.
Examination & Rehab Efforts
When a patient presents with pain post-vasectomy, symptoms may worsen with prolonged sitting, with pressure from clothing, or in association with sexual or fitness activities. Because there has been a local insult to the tissues, it is logical to check the site of the procedure for any breakdown, signs of significant inflammation, swelling, and to examine for signs of infection such as fever. (Most patients have returned to their medical provider once pain develops, but if they haven’t, a referral is appropriate.) If the pain can be reproduced locally at the site of the procedure, the pain can often be managed by local treatment. You might find benefit in exam procedures such as a trunk or hip extension for the soft tissue tensioning as well as mechanical loading; palpation to the abdominal wall as well as within the spermatic cord. Treatment can address guarding of the area, general wellness (nutrition, movement, mental health), simple modalities such as heat, and gentle self-mobilization to the painful area.
Granulomas
Granulomas can form following a vasectomy, and while usually asymptomatic, a granuloma may be responsible for post-vasectomy pain. They are described as a “bag-like” structure with disintegrating spermatozoa that form at the cut ends of a vasectomy. (Chatterjee et al., 2001) If the granuloma is painful, very light manual mobilization of the thickened area may be done to alleviate pain (see image below). Mobilization of the spermatic cord itself via the testicle or more proximally may also prove helpful. Local modalities such as ultrasound or heat may improve symptoms as well, but clinically I have found that gentle manual therapy and movement exercises are enough to resolve the pain within a few weeks. Patients can be instructed to complete self-mobilization to the area of the granuloma, and as they often are scared to touch the area, helping alleviate this fear is useful in healing.

Post-vasectomy syndrome is very challenging for patients to manage, as they are often dismissed once the procedure is completed. Patients will share that they have been told “everything looks healed” and that the pain should go away on its own. Most providers are unaware of the role of pelvic rehab clinicians, and many pelvic rehab providers are less knowledgeable about conditions related to the scrotum and spermatic cord. For patients who do not respond to conservative intervention, vasectomy reversals have been found to be significantly helpful in reducing pain, though it’s often undesired due to the goal of contraception that inspired the vasectomy. (Herrel et al., 2015; Polackwith et al., 2015). Ideally, patients will be provided with an early recommendation to pelvic rehab so that further procedures or undoing of the vasectomy is avoided.
If you’d like to learn more about post-vasectomy syndrome and many other conditions that can go unrecognized and under-treated, the next opportunity to take the Male Pelvic Floor course is coming up July 9-10,2021!
Chatterjee, S., Rahman, M. M., Laloraya, M., & Pradeep Kumar, G. (2001). Sperm disposal system in spermatic granuloma: a link with superoxide radicals. International journal of andrology, 24(5), 278-283.
Herrel, L. A., Goodman, M., Goldstein, M., & Hsiao, W. (2015). Outcomes of microsurgical vasovasostomy for vasectomy reversal: a meta-analysis and systematic review. Urology, 85(4), 819-825.
Lee, J. Y., Chang, J. S., Lee, S. H., Ham, W. S., Cho, H. J., Yoo, T. K., ... & Lee, S. W. (2012). Efficacy of vasectomy reversal according to patency for the surgical treatment of postvasectomy pain syndrome. International journal of impotence research, 24(5), 202-205.
Leslie, T.A., R.O. Illing, D.W. Cranston, J. Guillebaud (2007). “The incidence of chronic scrotal pain after vasectomy: a prospective audit.” BJU International 100: 1330-1333.
Polackwich, A. S., Tadros, N. N., Ostrowski, K. A., Kent, J., Conlin, M. J., Hedges, J. C., & Fuchs, E. F. (2015). Vasectomy reversal for postvasectomy pain syndrome: a study and literature review. Urology, 86(2), 269-272.
By accepting you will be accessing a service provided by a third-party external to https://www.hermanwallace.com/
All Upcoming Continuing Education Courses

Menopause Transitions and Pelvic Rehab - Remote Course - January 17 - 18 2026
Jan 17 2026 - Jan 18 2026

Pelvic Function Level 1 - Satellite - Bethpage NY - January 24 - 25 2026- SOLD OUT
Jan 24 2026 - Jan 25 2026

Pelvic Function Level 2B - Satellite - Port St. Lucie FL - January 24 - 25 2026
Jan 24 2026 - Jan 25 2026

Pelvic Function Level 1 - Satellite - Woodbury NY - January 24 - 25 2026 - SOLD OUT
Jan 24 2026 - Jan 25 2026

Pelvic Function Level 2B - Satellite - Torrance CA - January 24 - 25 2026 - SOLD OUT
Jan 24 2026 - Jan 25 2026

Pelvic Function Level 2B - Satellite - Indianapolis IN - January 24 - 25 2026 - SOLD OUT
Jan 24 2026 - Jan 25 2026


Pelvic Function Level 2B - Satellite - St. Augustine FL - January 24 - 25 2026
Jan 24 2026 - Jan 25 2026


Pelvic Function Level 1 - Satellite - Bradenton FL - January 24 - 25 2026 - SOLD OUT
Jan 24 2026 - Jan 25 2026

Pelvic Function Level 1 - Satellite - New York NY - January 24 - 25 2026 - SOLD OUT
Jan 24 2026 - Jan 25 2026

Pelvic Function Level 1 - Satellite - Los Angeles CA - January 24 - 25 2026 - SOLD OUT
Jan 24 2026 - Jan 25 2026





Pelvic Function Level 1 - In-Person - Columbus OH - January 31 - February 1 2026
Jan 31 2026 - Feb 1 2026

Pelvic Function Level 2C - Satellite - Boston MA - January 31 - February 1 2026
Jan 31 2026 - Feb 1 2026

Pelvic Function Level 2C - Satellite - Omaha NE - January 31 - February 1 2026
Jan 31 2026 - Feb 1 2026


Pelvic Function Level 1 - Satellite - Fairfax VA - February 7 - 8 2026 - SOLD OUT
Feb 7 2026 - Feb 8 2026

Pelvic Function Level 1 - Satellite - Queens NY - February 7 - 8 2026 - SOLD OUT
Feb 7 2026 - Feb 8 2026




Pelvic Function Level 1 - Satellite - Greenwich Village NY - February 7 - 8 2026 - SOLD OUT
Feb 7 2026 - Feb 8 2026



Pelvic Function Level 2B - Satellite - Seattle WA - February 14 - 15 2026 - SOLD OUT
Feb 14 2026 - Feb 15 2026

Pelvic Function Level 2B - Satellite - Galloway NJ - February 14 - 15 2026
Feb 14 2026 - Feb 15 2026

Pelvic Function Level 2B - Satellite - Owensboro KY - February 14 - 15 2026
Feb 14 2026 - Feb 15 2026
Mobilization of Visceral Fascia: Urinary - Satellite Lab Course - Torrance CA - February 20 - 22 2026
Feb 20 2026 - Feb 22 2026

Mobilization of Visceral Fascia: The Urinary System Satellite Lab Course - Self-Hosted - February 20 - 22 2026
Feb 20 2026 - Feb 22 2026

Mobilization of Visceral Fascia: Urinary - Satellite Lab Course - Lake Stevens WA - February 20 - 22 2026
Feb 20 2026 - Feb 22 2026

Mobilization of Visceral Fascia: Urinary - Satellite Lab Course - Medford OR - February 20 - 22 2026
Feb 20 2026 - Feb 22 2026



Pelvic Function Level 1 - Satellite - Nashville TN - February 21 - 22 2026
Feb 21 2026 - Feb 22 2026

Pain Science for the Chronic Pelvic Pain Population - Remote Course - February 21 - 22 2026
Feb 21 2026 - Feb 22 2026

Pelvic Function Level 1 - In-Person - Grand Rapids MI - February 21 - 22 2026
Feb 21 2026 - Feb 22 2026