September is Gynae Cancer Awareness Month
September is Gynae Cancer Awareness Month – but how aware are we as clinicians of the signs and symptoms, the epidemiology and the sequalae of treatment afterwards? As pelvic rehab specialists, we have the privilege of helping women live well after cancer treatment ends, both on a ‘local’ pelvic area (bladder, bowel, sexual and pelvic pain management strategies) but also on a more ‘global’ level – dealing with issues such as cancer related fatigue, bone health and cardiovascular concerns.
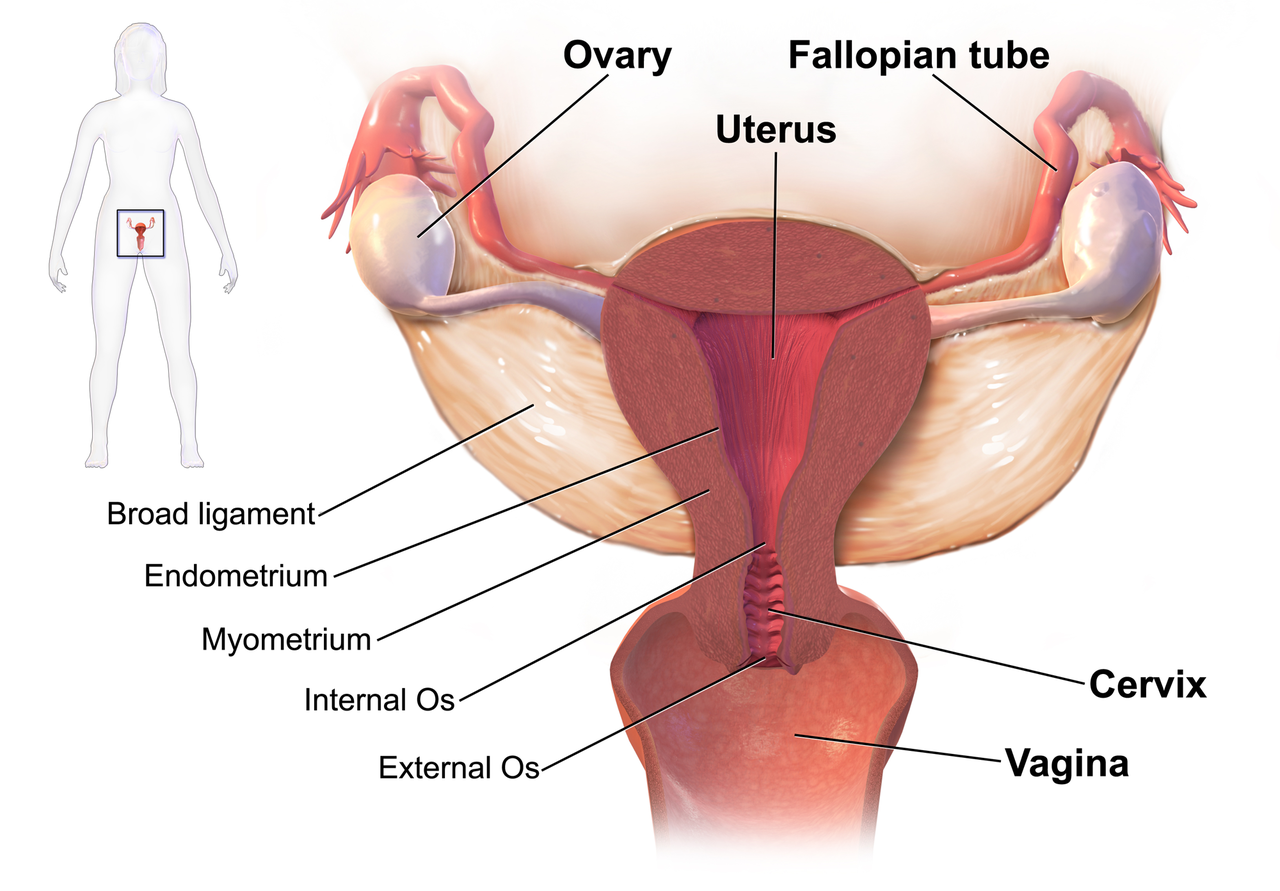 We know that women who are diagnosed with cancer of the vulva, vagina, cervix, endometrium or ovaries are treated with a combination of surgery, radiation or chemotherapy. However, with improving treatment and better survival rates, there is evidence that a variety of pelvic health concerns may arise for these women, both during and after treatment. (Hazewinkel et al 2010). For example, urinary incontinence is reported in 80% of women treated for endometrial cancer, with more severe symptoms and impact on quality of life in those who had adjuvant radiation (Erekson et al 2009) In Malone’s 2017 paper, ‘The patient’s voice: What are the views of women on living with pelvic floor problems following successful treatment for pelvic cancers?’, the author notes that ‘…there is currently a lack of knowledge regarding the effects of PFD on QoL in this cohort. Patients do not always report these problems to their health care providers and clinicians may underestimate symptoms…In the context of having survived cancer, PFD may be seen as relatively trivial. However, in the context of resuming normal living, the symptoms experienced by the survivors may be significant’.
We know that women who are diagnosed with cancer of the vulva, vagina, cervix, endometrium or ovaries are treated with a combination of surgery, radiation or chemotherapy. However, with improving treatment and better survival rates, there is evidence that a variety of pelvic health concerns may arise for these women, both during and after treatment. (Hazewinkel et al 2010). For example, urinary incontinence is reported in 80% of women treated for endometrial cancer, with more severe symptoms and impact on quality of life in those who had adjuvant radiation (Erekson et al 2009) In Malone’s 2017 paper, ‘The patient’s voice: What are the views of women on living with pelvic floor problems following successful treatment for pelvic cancers?’, the author notes that ‘…there is currently a lack of knowledge regarding the effects of PFD on QoL in this cohort. Patients do not always report these problems to their health care providers and clinicians may underestimate symptoms…In the context of having survived cancer, PFD may be seen as relatively trivial. However, in the context of resuming normal living, the symptoms experienced by the survivors may be significant’.
This can present a clinical conundrum – often pelvic rehab therapists are nervous when working with a patient who has a current or previous gynecologic cancer diagnosis, but similarly oncology rehab specialists may have qualms about dealing with pelvic health issues, with the result that these women fall through the cracks and do not have their pelvic health issues managed properly (or at all). Theodore Roosevelt once said ‘No one cares how much you know, until they know how much you care’ and this is especially relevant for oncology pelvic rehab. Often you may be the first clinician to ask about bladder, bowel or sexual function or dysfunction. An understanding of the effects of cancer treatments on the pelvis is important but so too is the wealth of information you may already have about bladder, bowel and sexual health as well as neuroscience and pain education.
The most important thing is to ask these women about their pelvic health concerns – the National Coalition for Cancer Survivorship defined cancer survivorship as extending from ‘the time of diagnosis and for the balance of life’. An emphasis on quality of life has been emphasised – if we know that cancer survivors may not independently volunteer information about their pelvic floor dysfunction, it is our responsibility to ask the questions and comprehensively treat and advocate for these women, in order to help them live well after cancer treatment ends.
- Hazewinkel MH. Sprangers MA, Velden Jvd, Vaart CH, Stalpers LJ, Burger MP ‘Longterm cervical cancer survivors suffer from pelvic floor dysfunction symptoms: A cross-sectional matched cohort study’ Gynecol Oncol 2010;117(2):381-6
- Erekson EA, Sung VW, Disilvestro PA, Myers DL ‘Urinary symptoms and impact on quality of life in women after treatment for endometrial cancer’ Int Urogynecol J 2009;20(2):159-63
- Malone P, Danaher D, Galvin R, Cusack T ‘The patient’s voice: What are the views of women on living with pelvic floor problems following successful treatment for pelvic cancers?’ Physiotherapy Practice and Research 38(2017)93-102
By accepting you will be accessing a service provided by a third-party external to https://www.hermanwallace.com/
All Upcoming Continuing Education Courses

Pelvic Function Level 1 - Satellite - Torrance CA - June 14 - 15 2025 - SOLD OUT
Jun 14 2025 - Jun 15 2025

Pelvic Function Level 1 - Satellite - Long Beach CA - June 14 - 15 2025 - SOLD OUT
Jun 14 2025 - Jun 15 2025

Pelvic Function Level 1 - Satellite - Woodbury NY - June 14 - 15 2025 - SOLD OUT
Jun 14 2025 - Jun 15 2025

Pelvic Function Level 1 - Satellite - Leavenworth KS - June 14 - 15 2025 - SOLD OUT
Jun 14 2025 - Jun 15 2025

Pelvic Function Level 1 - Satellite - New York NY - June 14 - 15 2025 - SOLD OUT
Jun 14 2025 - Jun 15 2025

Pain Science for the Chronic Pelvic Pain Population - Remote Course - June 21 - 22 2025
Jun 21 2025 - Jun 22 2025

Dry Needling and Pelvic Health - In-Person - Atlanta GA - June 21 - 22 2025 - SOLD OUT
Jun 21 2025 - Jun 22 2025



Mobilization of Visceral Fascia - Gastrointestinal - Satellite Lab Course - St. Petersburg FL - June 27 - 29 2025
Jun 27 2025 - Jun 29 2025

Mobilization of Visceral Fascia - Gastrointestinal - Satellite Lab Course - Self-Hosted - Jun 27 - 29 2025
Jun 27 2025 - Jun 29 2025

Mobilization of Visceral Fascia - Gastrointestinal - Satellite Lab Course - Sellersville PA - June 27 - 29 2025
Jun 27 2025 - Jun 29 2025

Mobilization of Visceral Fascia - Gastrointestinal - Satellite Lab Course - Milwaukee WI - June 27 - 29 2025
Jun 27 2025 - Jun 29 2025

Mobilization of Visceral Fascia - Gastrointestinal - Satellite Lab Course - Medford OR - June 27 - 29 2025
Jun 27 2025 - Jun 29 2025

Mobilization of Visceral Fascia - Gastrointestinal - Satellite Lab Course - Bartlett IL - June 27 - 29 2025
Jun 27 2025 - Jun 29 2025

Mobilization of Visceral Fascia - Gastrointestinal - Satellite Lab Course - Cedar Knolls NJ - June 27 - 29 2025
Jun 27 2025 - Jun 29 2025

Mobilization of Visceral Fascia - Gastrointestinal - Satellite Lab Course - Marysville OH - June 27 - 29 2025
Jun 27 2025 - Jun 29 2025

Mobilization of Visceral Fascia - Gastrointestinal - Satellite Lab Course - New Orleans LA - June 27 - 29 2025
Jun 27 2025 - Jun 29 2025

Mobilization of Visceral Fascia - Gastrointestinal - Satellite Lab Cource - Amherst OH - June 27 - 29 2025
Jun 27 2025 - Jun 29 2025

Mobilization of Visceral Fascia - Gastrointestinal - Satellite Lab Cource - Paso Robles CA - June 27 - 29 2025
Jun 27 2025 - Jun 29 2025



Pelvic Function Level 1 - Satellite - Tampa FL - June 28 - 29 2025 - SOLD OUT
Jun 28 2025 - Jun 29 2025


Pelvic Function Level 1 - Satellite - Waco TX - June 28 - 29 2025 - SOLD OUT
Jun 28 2025 - Jun 29 2025



Pelvic Function Level 1 - Satellite - Milwaukee WI - July 12 - 13 2025 - SOLD OUT
Jul 12 2025 - Jul 13 2025

Modalities and Pelvic Function - In-Person - Houston TX - July 12 - 13 2025
Jul 12 2025 - Jul 13 2025

Pelvic Function Level 1 - Satellite - Denver CO - July 12 - 13 2025 - SOLD OUT
Jul 12 2025 - Jul 13 2025

Pelvic Function Level 2B - Satellite - Sellersville PA - July 19 - 20 2025
Jul 19 2025 - Jul 20 2025



Pelvic Function Level 1 - Satellite - Des Moines IA - July 26 - 27 2025 - SOLD OUT
Jul 26 2025 - Jul 27 2025

Pelvic Function Level 1 - Satellite - Minneapolis MN - July 26 - 27 2025 - SOLD OUT
Jul 26 2025 - Jul 27 2025

Pelvic Function Level 1 - Satellite - St. Augustine FL - July 26 - 27 2025
Jul 26 2025 - Jul 27 2025

Pelvic Function Level 1 - Satellite - Virginia Beach VA - July 26 - 27 2025 - SOLD OUT
Jul 26 2025 - Jul 27 2025


Dry Needling and Pelvic Health 2 - In Person - Duluth MN - August 2 - 3 2025
Aug 2 2025 - Aug 3 2025