



At Herman & Wallace, we know that pelvic rehabilitation is a dynamic and ever-evolving field. While foundational courses like Pelvic Function Level 1 and Dry Needling and Pelvic Health often get the spotlight, there are several highly valuable courses that tend to fly under the radar. These courses offer practitioners the opportunity to deepen their knowledge, broaden their skills, and better serve patients with complex needs.
Here are five underrated courses that can have a powerful impact on your practice:
1. Nutrition Perspectives for the Pelvic Rehab Therapist
Pelvic health doesn’t exist in isolation from the rest of the body, and nutrition plays a critical role in tissue healing, inflammation, digestion, and pelvic pain syndromes. This course introduces pelvic rehab practitioners to the fundamentals of nutrition as it relates to pelvic health.
Working with children in pelvic rehabilitation is a deeply meaningful and highly specialized area of practice. It also comes with unique ethical responsibilities. Pediatric pelvic health involves treating conditions such as enuresis, constipation, pelvic floor dysfunction, and developmental delays — all within the context of a child’s developing autonomy, family dynamics, and sensitive anatomical areas.
As clinicians, our ethical frameworks must evolve to accommodate not only clinical best practices but also the emotional, developmental, and psychosocial needs of the child.
Here, we examine the critical ethical principles that should guide our work in pediatric pelvic rehab.
Coccydynia, commonly referred to as tailbone pain, can be a profoundly limiting and misunderstood condition. Although it affects a relatively small percentage of patients, its impact on function and quality of life is often disproportionate to its size. As pelvic rehabilitation therapists, we are uniquely positioned to assess and treat the biomechanical, musculoskeletal, and neuromuscular contributors to coccydynia, especially when sitting becomes painful or intolerable.
Coccydynia is typically defined as pain in the coccyx region, often exacerbated by sitting, transitioning from sit to stand, or activities that increase pressure on the tailbone (e.g., biking or prolonged driving). While trauma, like a fall onto the tailbone or childbirth, is a common cause, many cases are idiopathic or associated with repetitive strain, postural dysfunction, or referred pain from nearby structures.
Some key contributors we see in clinical practice include coccygeal hypermobility or hypomobility, myofascial dysfunction (in pelvic floor muscles, gluteal, obturator internus, or levator ani muscles), lumbar/sacral or SI joint dysfunction, scarring or adhesions from previous surgeries or trauma, central sensitization, and chronic pain responses.
As pelvic rehabilitation therapists, we are uniquely positioned to deliver care that honors both the physical and emotional complexities of each patient's body. Our field often involves working intimately with anatomy, which means it's essential to provide affirming, informed, and inclusive care for all individuals, including those who are intersex.
The intersection of pelvic rehabilitation and intersex health demands not only biomechanical insight but also a sophisticated, embodied understanding of trauma, identity, and consent. As clinicians working within the intimate landscapes of the pelvis, we must widen our therapeutic lens to serve the needs of intersex individuals — those born with variations that fall outside binary definitions of male or female bodies.
Intersex variations (sometimes referred to as DSDs, or differences of sex development — though this term remains controversial) include a wide spectrum of chromosomal, gonadal, hormonal, and anatomical variations. These include, but are not limited to: Androgen Insensitivity Syndrome (AIS), Congenital Adrenal Hyperplasia (CAH), Klinefelter syndrome (XXY), Turner syndrome (XO), 5-Alpha-Reductase Deficiency, and mixed gonadal dysgenesis.
As pelvic rehabilitation continues to evolve, so does our understanding of how to access and modulate the intricate neuromuscular systems that govern pelvic floor function.
Dry needling — long employed in orthopedic and sports medicine settings — is now emerging as a potent tool in the pelvic health therapist’s repertoire. Its precise application can yield neurophysiologic effects far beyond simple trigger point release, particularly when integrated with a broader neuromodulation framework.
As pelvic rehabilitation therapists, our role has traditionally focused on restoring continence, alleviating pain, and improving quality of life. Yet within athletic populations, pelvic floor dysfunction often presents in unique and nuanced ways—masked by high levels of conditioning, normalized symptoms, or misattributed pain patterns. As the bridge between performance and pelvic health, we are uniquely positioned to address these challenges.
In athletes, the pelvic floor must do more than support visceral structures or maintain continence. It plays an integral role in force transmission, lumbopelvic stability, breathing mechanics, and reflexive motor control. The demands of sport—sprinting, lifting, jumping, cutting—place high, repetitive loads on the core system, often revealing (or creating) dysfunctions in timing, tone, and coordination of the pelvic floor.
The athletic population requires a different lens: one that views the pelvic floor as a functional component of the kinetic chain and not in isolation.
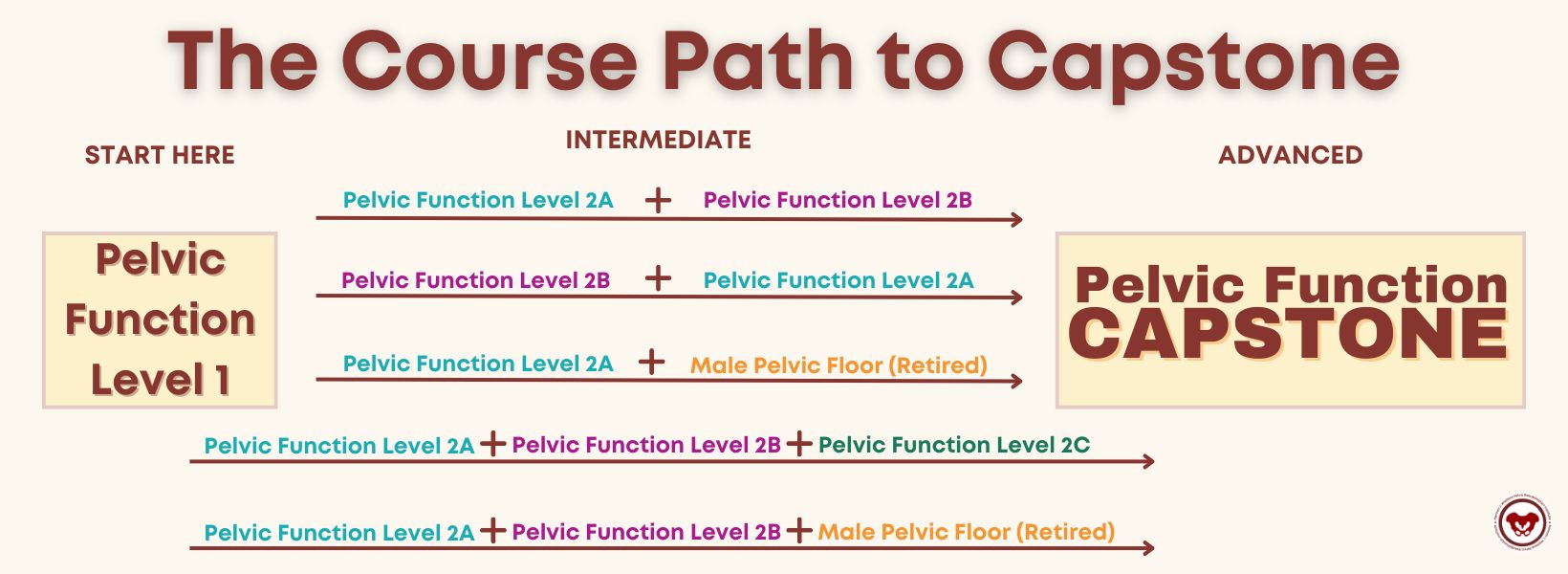
Most practitioners know that Capstone is the advanced level course that caps off the Pelvic Function Series. This article covers two main questions:
- Why should you aspire to Capstone?
- What is the course path to Capstone?
- Where do you go after Capstone?
Why should you aspire to Capstone?
If you are new to pelvic rehabilitation or an experienced practitioner, you should think about taking Pelvic Function Capstone. For beginner practitioners who are interested in completing the Pelvic Function Series, the Capstone path will take you from the introductory Pelvic Function Level 1, where you learn intra-vaginal exam techniques, through Pelvic Function Level 2A, which includes an introduction to anorectal examination. AND you can tailor your course journey to your patient demographics.
Congratulations on completing Pelvic Function Level 1 (PF1) and entering the world of pelvic rehabilitation. Are you ready for your next course but not quite sure which one to take? Well, you’re not alone. Everyone’s pelvic health educational journey is different based on their interests and patient demographics and there are a lot of course options available.
I’m going to zero in on the intermediate-level courses in the Pelvic Function Series for you as HW does recommend that practitioners take at least one or two of these. If you’ve looked at the course page you’ve noticed that there are three courses with a Level 2 designation – as well as a lab course. What does this mean? These courses are designed to be a progression of knowledge and skills learned in the foundational course Pelvic Function Level 1.
Here are the intermediate courses:
Herman & Wallace offers a number of downloadable products on our website for your clinical practice, and we want to put you in charge of deciding which new products we create and offer!
What is a Prefund?
The HW philosophy is that we should only be making products that are useful to our practitioners. In our efforts to create the most valuable products and keep the price as low as possible, we have launched a new Prefund product development program.
Need more information? Check out the Prefund FAQs.


Do you listen to any podcasts? What about podcasts that are focused on pelvic issues and aimed toward the pelvic health practitioner? Here at Herman & Wallace, many of us listen to these and we all have our favorites. Recently HW was lucky enough to work with The Pelvic Service Announcement when Callie and Rachel interviewed Holly Tanner for the episode “Stay Curious and Stay Open” which is available on streaming platforms today.
Who are Callie Teel and Rachel Fritz?
Callie and Rachel are two physical therapists whose passion for women’s health and commitment to education are changing the way people think about this important field.
Callie and Rachel first crossed paths at Texas Tech University Health Sciences Center, where they both graduated from physical therapy school in 2021. Following their graduation, the duo began their careers at Optimal Physical Therapy in Amarillo, Texas. It didn't take long for them to realize that there was a significant gap in the public's understanding of pelvic health and the role of pelvic floor physical therapy.
All Upcoming Continuing Education Courses

Pelvic Function Level 1 - Satellite - Milwaukee WI - July 12 - 13 2025 - SOLD OUT
Jul 12 2025 - Jul 13 2025

Modalities and Pelvic Function - In-Person - Houston TX - July 12 - 13 2025
Jul 12 2025 - Jul 13 2025

Pelvic Function Level 1 - Satellite - Denver CO - July 12 - 13 2025 - SOLD OUT
Jul 12 2025 - Jul 13 2025




Pelvic Function Level 1 - Satellite - Des Moines IA - July 26 - 27 2025 - SOLD OUT
Jul 26 2025 - Jul 27 2025

Pelvic Function Level 1 - Satellite - Minneapolis MN - July 26 - 27 2025 - SOLD OUT
Jul 26 2025 - Jul 27 2025

Pelvic Function Level 1 - Satellite - St. Augustine FL - July 26 - 27 2025
Jul 26 2025 - Jul 27 2025

Pelvic Function Level 1 - Satellite - Virginia Beach VA - July 26 - 27 2025 - SOLD OUT
Jul 26 2025 - Jul 27 2025


Pelvic Function Level 1 - In-Person - Chicago IL - August 2 - 3 2025 - SOLD OUT
Aug 2 2025 - Aug 3 2025



Menopause Transitions and Pelvic Rehab - Remote Course - August 9 - 10 2025
Aug 9 2025 - Aug 10 2025









Pelvic Function Level 2C - Satellite - Palm Beach FL - August 16 - 17 2025
Aug 16 2025 - Aug 17 2025

Pelvic Function Level 2C - Satellite - New Orleans LA - August 16 - 17 2025
Aug 16 2025 - Aug 17 2025

Pelvic Function Level 2C - Satellite - Paso Robles CA - August 16 - 17 2025
Aug 16 2025 - Aug 17 2025


Pediatrics Level 1 - Treatment of Bowel and Bladder Disorders - Remote Course - August 23 - 24 2025
Aug 23 2025 - Aug 24 2025

Pelvic Function Level 1 - Satellite - Jacksonville FL - August 23 - 24 2025
Aug 23 2025 - Aug 24 2025

Pelvic Function Level 1 - Satellite - Chicago IL - August 23 - 24 2025 - SOLD OUT
Aug 23 2025 - Aug 24 2025


Rehabilitative Ultrasound Imaging Pelvic Health Satellite Lab Course - Self-Hosted - September 5 - 7 2025
Sep 5 2025 - Sep 7 2025
Rehabilitative Ultrasound: Orthopedic Topics Satellite Lab Course - Self-Hosted - September 5 - 6 2025
Sep 5 2025 - Sep 6 2025

Rehabilitative Ultrasound Imaging Pelvic Health Satellite Lab Course - Indianapolis IN - September 5 - 7 2025
Sep 5 2025 - Sep 7 2025
Rehabilitative Ultrasound: Orthopedic Topics Satellite Lab Course - Indianapolis IN - September 5 - 6 2025
Sep 5 2025 - Sep 6 2025
