
Recently, the Institute was made aware of an internet scam that is targeting physical therapists, including members of our teaching faculty. A bogus website called ComplaintsBoard has listed many PTs, including several respected Herman & Wallace faculty members, on a list of convicted sexual abusers. This site contains a similar list of doctors and lawyers that it claims have criminal records, meaning that patients or clients seeking professionals may find false and damning histories on internet search engines. The site then invites those whose names are posted to pay money through a different website to clear their records.
Clearly, this is the work of scam artists that are tarnishing the reputations of physical therapists. It is unclear who these perpetrators are, but they have targeted a number of respected professionals, including members of our faculty. Herman & Wallace is dismayed to see the character of professionals with whom we work and respect being attacked for profit. The APTA has been made aware of this, and is seeking legal action. If you find your name on such a list, please contact the APTA.
The Institute would like to make our community aware of this problem and to show our support of our faculty and our colleagues.
Please understand that, because we do not want to increase the web traffic to these scam sites, thereby increasing their efficacy, we will not be posting direct links to these sites.
A colleague recently sent an inquiry through the Institute asking if there is new research supporting pelvic floor muscle training after radical prostatectomy. As a matter of fact, I chose not to report on some recent research that I read, because it does not support conservative care for urinary incontinence (UI). The Cochrane review for postprostatectomy UI was updated this year, and the results of the review indicate that we need more and better research. (If you are unfamiliar with the Cochrane library, one of its 6 databases contains systematic reviews of the literature that are updated periodically.) Although within the abstract of the reviewthe report states that there is a lack of consistency in the interventions, the populations, and in the outcome measures, the value of conservative approaches is deemed "uncertain." The authors do conclude that benefit from one-to-one pelvic floor muscle training is "unlikely" following transurethral resection of the prostate, or TURP.
The critiques of the research listed in the review include the above mentioned lack of consistency in outcomes and interventions. Most of the studies also did not include a report of pre-surgical outcome status, of adverse effects, and lifestyle changes as an intervention was never identified in any of the research. This leads us to this question: why are we treating men for UI or erectile dysfunction (ED) if this systematic review brings into question the efficacy of what we do? Certainly patients are improving as a result of pelvic rehabilitation, or I doubt that the medical providers would continue to refer patients to the offices who provide rehabilitation to these patients. What we do not know about each of the studies is how much of the male anatomy was affected by the procedure for the prostate. The patient's pre-surgical status and the skill level of the surgeon are both known factors for outcomes following prostatectomy, yet how are those quantified in the literature?
Most importantly, how can we be a part of the solution when it comes to creating research to support the services that we provide. It may be helpful as therapists to be certain that we are maximizing the level of knowledge about the surgeries, the anatomy involved, and about the available treatments. This can mean attending coursework that is specific to or includes discussion of male pelvic floor issues. (Check out the Pelvic Floor Series level 2A course or the Male Pelvic Floor Courses offered by the Institute, especially if more male patients are finding their way to your door.) Speak with referring physicians about surgical techniques, observe some surgeries, or attend a urology conference (maybe there's one near your hometown, or you want to attend with your local referring urology group.) Always document using outcomes studies when you can. Write a case study. You can even purchase a text book that teaches you step-by-step how to write a case study. I know that you don't have time...so, create a weekly lunch meeting at work with a colleague where you each work on and critique each other's project. Getting involved with local university programs can also allow you to be part of the research solution.
In summary, we need more and better research that documents how we are helping our patients. In relation to male patients following prostate procedures, who is screening these men to decide if they have tight, painful pelvic floor muscles versus weak muscles with lack of awareness of their use? We are the best chance the patient has in helping with the rehabilitation process. It is also imperative that we are testing muscle function in men to help categorize the patient as someone who might improve with an exercise-based approach or as someone who might need a trial of pelvic floor muscle electrical stimulation. If you tend to complete internal muscle testing with women, yet feel uncomfortable with this approach in men, I encourage you to move forward in your practice of this critical skill. We need to catch the patients early on who seem to have no muscle function and no awareness, and then refer that patient back to the surgeon within a reasonable time frame if there is a lack of progress. A few of the men I worked with who went on to have a male sling had very positive outcomes, and they also were very grateful that they had a pelvic rehabilitation provider to give guidance and feedback along the way. Patients who are more aware of their pelvic muscles, how to use them (and not use them!), and who know how to take care of their pelvic muscles throughout their lifespan are better poised to handle the post-surgical pathway if they should require further intervention.

Today, September 28th, marks the ten year anniversary of the founding of Herman & Wallace! The Institute was founded on this day in 2005 by Holly Herman, PT, DPT, MS, OCS, WCS, BCB-PMD, PRPC and Kathe Wallace, PT, BCB-PMD with a mission of providing the very best evidence-based continuing education related to pelvic floor and pelvic girdle dysfunction in men and women throughout the life cycle.
Since our founding, it’s been our privilege to spread this mission through an ever-increasing number of course offerings, products, resources and certification so that therapists can meet their goals and patients can access trained practitioners who can address their needs.
To celebrate with us, use the discount code HappyBirthday for $10 off your next downloadable Herman & Wallace product!
In the past ten years, we’ve significantly expanded our course offerings. Currently-offered courses cover pediatrics and geriatrics, sexual health, yoga and Pilates, oncology, meditation and mindfulness, and a number of other topics instructed by some of the foremost experts in the field, with whom we are thrilled to work and provide a platform to spread their knowledge. In addition to our flagship Pelvic Floor series courses which were the first offered by the Institute, H&W now offers 46 live courses and 14 online courses on topics related to pelvic floor dysfunction, as well as related women’s health, men’s health and orthopedic topics.
We have also had the opportunity to take this mission abroad and have offered pelvic floor courses in Saudi Arabia, United Arab Emirates, Chile, Brazil, the UK and Europe. In 2013, H&W launched the first-ever certification recognizing expertise in treating pelvic floor dysfunction in men and women throughout the life cycle, the Pelvic Rehabilitation Practitioner Certification. Since then, 84 practitioners have sat for and passed this exam and earned PRPC as a designation of their competence in evaluating and treating pelvic rehab patients. This coming year and beyond, we are looking forward to continuing with our mission of providing the very best education and resources for pelvic rehab therapists. We are continuing to expand our offerings of intermediate and advanced- level Pelvic Floor coursework for experienced therapists, as well as an increasing number of scheduled events for our introductory courses so that more practitioners can begin learning the skills needed to serve this growing patient population.
Over these years, the best part is hearing from therapists that our mission is changing lives for practitioners and for patients. This recent email we received from a course participant is the best birthday gift we received!:
“I always gain so much from your courses and they are the first ones I look to each year for simply excellent use of my education dollars and to further my knowledge of Women’s/Men’s/Children’s Pelvic Health. Kuddo’s to you, sincerely, for really making a difference in the lives of so many – that you, as therapists, work with directly, AND that you “work with” through each therapist that you train. What a huge ripple effect for making the difference in the lives of many…..and on such personal issues. And I give due credit to you with each patient I see for the training I have and am still receiving! Thank-you!!!!”
![]() The Herman & Wallace Pelvic Rehabilitation Institute was founded nearly a decade ago by physical therapists and educators Kathe Wallace and Holly Herman. The Institute has served as a platform for foundational to advanced pelvic rehabilitation coursework that covers a wide variety of topics. Included in some of the newer coursework is content directed at more general orthopedics or women’s health topics, such as:
The Herman & Wallace Pelvic Rehabilitation Institute was founded nearly a decade ago by physical therapists and educators Kathe Wallace and Holly Herman. The Institute has served as a platform for foundational to advanced pelvic rehabilitation coursework that covers a wide variety of topics. Included in some of the newer coursework is content directed at more general orthopedics or women’s health topics, such as:
- Biomechanical Assessment of the Hip and Pelvis
- Rehabilitative Ultrasound Imaging: Orthopedic Topics
- Physical Therapy for the Breast Oncology Patient
- Neck Pain, Headaches, Dizziness, and Vertigo
- Manual Therapy for the Lumbo-Pelvic-Hip Complex.
Occasionally, as we have continued to expand our offerings at the Institute, participants have expressed concern that a few of the courses are “not pelvic floor” related. We wanted to take a moment to share our perspective regarding that concern:
1. Most pelvic rehabilitation providers are not exclusively working with patients who have pelvic floor dysfunction.
When we completed a survey of job task analysis among pelvic rehabilitation therapists, we learned that many therapists are not working with patients who have pelvic dysfunction 100% of their time, and that general musculoskeletal care makes up a large part of many pelvic rehab therapists’ caseload. Unfortunately, many patients aren’t often dealing with only one dysfunction, so our patients who present with urinary incontinence may also have foot pain, or headaches, for example.
2. Many pelvic rehabilitation providers also describe themselves as orthopedic therapists.
The majority of therapists who responded to our job analysis survey (and those who attend our courses) work in either an outpatient facility or a hospital-based outpatient facility. In fact, many of the respondents are board-certified in orthopedics. Outpatient facilities typically require that a therapist can work with any part of the body, in addition to the pelvis.
3. General orthopedic rehabilitation is closely related to pelvic rehabilitation.
There are an overwhelming number of ways that a patient’s comorbid conditions can be related to the pelvic floor. For example, a patient with foot pain may unload the involved side, placing increased strain on the hip, pelvis, and low back on the opposite side. Another patient who has poor balance may decrease their degrees of freedom by holding the trunk and pelvic muscles tense in order to compensate for a balance difficulty. A patient who has migraines may have to spend a significant amount of time lying flat when she has migraines, potentially leading to discomfort in other joints.
4. We have not decreased the amount of pelvic courses we offer in exchange for general, orthopedic courses. On the contrary, the Institute has continued to add more focused pelvic rehabilitation courses such as Post-Prostatectomy Patient Rehabilitation, Assessing and Treating Women with Vulvodynia, and Geriatric Pelvic Floor Rehab.
In short, we have chosen to offer some coursework that is not solely focused on the pelvis, because these courses can provide benefits to the therapists and to the patients they serve. The Institute is always interested in participant feedback, and is willing to try out new courses to gauge interest level and satisfaction with new courses. As always, you will be provided with the best in pelvic rehabilitation education, and have opportunities to take courses from instructors who offer additional skills and expertise. If you have any questions, or suggestions about course content, please let us know by filling out the Contact Us form on the website. And if you have an idea for a new course you’d like to teach that adds to our existing offerings, we’d love to hear from you- please fill out this form if you have a new course idea.

Patients who suffer severe bladder damage or bladder disease such as invasive cancer may have the entire bladder removed in a cystectomy procedure. Once the bladder is removed, a surgeon can use a portion of the patient's ileum (the final part of the small intestines) or other part of the intestine to create a pouch or reservoir to hold urine. This procedure can be done using an open surgical approach or a laparoscopic approach. Once this new pouch is attached to the ureters and to the urethra, the "new bladder" can fill and stretch to accommodate the urine. As the neobladder cannot contract, a person will use abdominal muscle contractions along with pelvic floor relaxation to empty. If a person cannot empty the bladder adequately, a catheter may need to be utilized. (A prior blog post reported on potential complications of and resources for learning about neobladder surgery.)
During the recovery from surgery, patients will wear a catheter for a few weeks while the tissues heal. Once the catheter has been removed, patients may be instructed to urinate every 2 hours, both during the day and at night. Because patients will not have the same neurological supply to alert them of bladder filling, it will be necessary to void on a timed schedule. The time between voids can be lengthened to every 3-4 hours. Night time emptying may still occur up to two times/evening. Patient recommendations following the procedure may include that patients drink plenty of fluids, eat a healthy diet, and gradually return to normal activities. Adequate fluid is important in helping to flush mucous that is in the urine. This mucous is caused by the bowel tissue used to create the neobladder, and will reduce over time.
Urinary leakage is more common at night in patients who have had the procedure, and this often improves over a period of time, even a year or two after the surgery. As pelvic rehabilitation providers, we may be offering education about healthy diet and fluid intake, pelvic and abdominal muscle health and coordination, function retraining and instruction in return to activities. In addition to having gone through a major surgical procedure, patients may also have experienced a period of radiation, other treatments, or debility that may limit their activity levels. The Pelvic Rehabilitation Institute is pleased to offer courses by faculty member Michelle Lyons in Oncology and the Pelvic Floor, Part A: Female Reproductive and Gynecologic Cancers, and Part B: Male Reproductive, Bladder, and Colorectal Cancers. If you would like to explore pelvic rehabilitation in relation to oncology issues, there is still time to register for the Part A course taking place in Torrance, California in May! If you would like to host either of these courses at your facility, let us know!
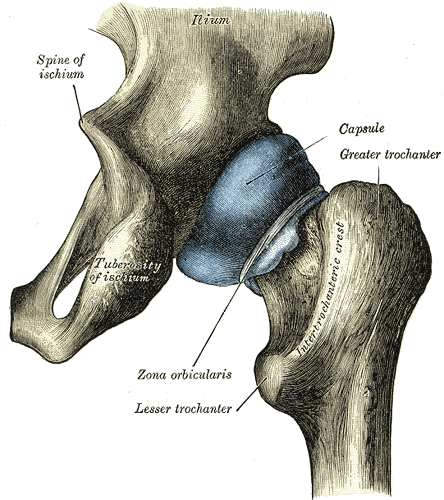
An article appearing this year in Arthroscopy details a systematic review completed to determine if asymptomatic individuals show evidence on imaging of femoroacetabular impingement, or FAI. Cam, pincer, and combined lesions were included in the results. To read some basics about femoroacetabular injury, click here. Over 2100 hips (57% men, 43% women) with a mean age of 25 were studied. (Only seven of the 26 studies reported on labral tears.) The researchers found the following prevalence in this asymptomatic population:
Cam lesion: 37% (55% in athletes versus 23% in general population)
Pincer lesion: 67%
Labral tears: 68%
Mean lateral and anterior center edge angles: 30-31 degrees
The authors conclude that femoroacetabular impingement tissue changes and hip labral injury are common findings in asymptomatic patients, therefore, clinicians must determine the relevance of the findings in relation to patient history and physical examination. Because hip pain is a common comorbidity of pelvic pain, knowing how to screen the hip joint for FAI or labral tears, rehabilitate hips with joint dysfunction, and help someone return to activity following a hip repair is valuable to the pelvic rehabilitation therapist.
As the athletic population may have increased risk of hip injuries due to overuse, traumatic injury, or vigorous activity, being able to address dysfunction in both high level and less active patients is necessary. Herman & Wallace faculty member Steve Dischiavi has developed a course rich in athletic examples and including education about activating fascial systems in various planes. If you are ready to step up your game related to Biomechanical Assessment of the Hip & Pelvis, check out this continuing education course taking place next in Durham, North Carolina in May.

If you area clinic owner, are in a management or leadership position, one of your jobs is making sure your therapists are using best practices. This can be a challenge when best practices are continually being researched and discussed, and when systematic reviews continue to tell us that pelvic rehabilitation research lacks homogeneity and enough high-level evidence to make convincing arguments about interventions. In the absence of this, we can still integrate recommendations from clinical practice guidelines and from best practice statements. The American Physical Therapy Association's (APTA) Section on Women's Health (SOWH) is participating in the APTA's initiative to develop clinical practice guidelines. For current guidelines, check out their page here. To see which guidelines are in development at the APTA, click here.

The American Urological Association (AUA) has also developed practice guidelines, including the Guideline on the Diagnosis and Treatment of Interstitial Cystitis/Bladder Pain Syndrome (IC/PBS). Within this guideline, the first line treatments are listed as general relaxation/stress management, pain management, patient education, and self-care/behavioral modification. Second-line treatments include "appropriate manual physical therapy techniques", oral medications, bladder medications (administered inside the bladder), and pain management. What is very interesting about this guideline is that the authors define what types of manual therapy approaches are appropriate, and these include techniques that resolve muscle tenderness, lengthen shortened muscles, release painful scars or other connective tissue restrictions. The guidelines also define who should be working with patients who have IC/PBS and pelvic muscle tenderness: "appropriately trained clinicians". Very importantly, the authors state that pelvic floor strengthening exercises should be avoided.
How can these guidelines be used to assess best practices? Find out if your therapists who work with patients who have IC/PBS are indeed instructing in relaxation strategies, using pain education and pain management techniques (for pain-brain education specific to pelvic pain, check out the book "Why Pelvic Pain Hurts". Find out if your therapist is instructing in pelvic muscle strengthening as a first-line of treatment, since this would not be in line with the AUA guidelines. (Having said this, teaching pelvic muscle strengthening can be very appropriate when done with consideration of pelvic muscle pain.) Lastly, ask your therapist if she feels that her skill set and training is sufficient to treat the condition. Even in our comprehensive pelvic floor series, there is so much to learn at the initial course that IC/PBS is not discussed in great detail until PF2B. Maybe a little more knowledge and training would help your therapist feel that she is providing the "appropriate manual physical therapy techniques" recommended in the guidelines.
To find out when the next intermediate or advanced course in the series is happening, or to find other specialty courses, check our course listings to see if there is a course happening near you!

Many diagnoses that live under the umbrella of "chronic pelvic pain" have similar symptoms, confounding the differential diagnosis and development of a treatment pathway. Dr. Charles Butrick, in an article published in 2007, suggested that gynecologists "…be alert to…interstitial cystitis in patients who present with chronic pelvic pain typical of endometriosis." The concurrent conditions of bladder pain syndrome (BPS) and endometriosis have been described as "evil twins syndrome" in the realm of chronic pelvic pain. Bladder pain syndrome. also known as Interstitial Cystitis (IC), is a condition commonly associated with pelvic pain, bladder pressure, and urinary dysfunction such as urgency and frequency. Endometriosis can also cause or contribute to pelvic pain, and a variety of pelvic dysfunctions including bowel, bladder, or sexual dysfunction.

A study published in the International Journal of Surgery reported on the prevalence of these two conditions. Utilizing a systematic review approach, the authors located articles reporting on the prevalence of bladder pain syndrome and endometriosis in women with chronic pelvic pain. Nine observational studies were included, and the range of endometriosis diagnosis ranged from 11%-97%, with a mean prevalence of 61%. The prevalence of endometriosis ranged from 28%-93% with a mean prevalence of 70%. The large variation in these rates were explained as potentially being due to the variations in study quality and sample selection. (The authors point out that the highest rates of prevalence for BPS and endometriosis were noted in the patient groups recruited from specialist clinics and from lists of patients from operating lists.) The study concludes that in women who present with chronic pelvic pain (CPP), screening for bladder pain syndrome is important so that appropriate treatment can be directed to all issues.
If another chronic pelvic pain condition, pudendal neuralgia, is added to the diagnoses of endometriosis and painful bladder syndrome, "evil triplet syndrome" can be experienced by a patient. The various symptoms of each of these conditions can add to the total level of pain and dysfunction experienced by a woman with chronic pelvic pain. Having the tools to evaluate and treat symptomatology and address the chronic aspect of tissue, joint, neural, myofascial, and the processing of pain is a skill that most pelvic rehabilitation therapists continue to work on throughout their careers. Michelle Lyons, faculty member from Ireland, brings her "Special Topics in Women's Health" course to Chicago in a couple of weeks. Within the course, Michelle will be discussing each of these conditions from the standpoint of a multidisciplinary approach, and with the role of the pelvic rehabilitation provider in mind. She will also be sharing up-to-date and practical information about infertility and hysterectomy. If you are interested in joining Michelle and colleagues in Chicago, you still have time to sign up! And if you would like to host Michelle's course in your facility, give us a call or send us a note!

Even after teaching for a couple of decades, both in graduate level courses and in continuing education settings (live and online), I am humbled by all there is to learn and relearn about how to teach well. We all teach every day, regardless of what setting or roles we work in, and are required to share our thoughts and knowledge with respect, equanimity, and non-judgement. After teaching a course last month, I received feedback about an important topic that was not clearly addressed from an instructional or clinical standpoint, and the participant who brought it to my attention agreed to share her experience so that we as pelvic rehab providers can do a better job of addressing the issue when needed. The following post was written by Erin B. after I encouraged her to share her own thoughts about the issue.
"Having recently participated in the PF1 class after several years out of the classroom-style of continuing education, I made a few observations I felt compelled to share. (I do want to preface this with the fact that I am fully aware that my own insecurities play a role in my experiences and I recognize that they may alter my judgment of the situation.)

I am 5' 4" and currently 240 pounds. Although that is 50 pounds lighter than I was 6 months prior to attending this class, it is still significantly larger than 90% of the class participants, lab assistants and instructors. I am not someone who feels that fat is healthy. I do not feel that you need to act like I am in as good of shape as anyone else in the room. However, I do feel that there are certain assumptions made about me that are based on my physical appearance alone. Take a minute and think about your first reaction to seeing a person who is obviously overweight. (I do realize that I have made my own assumptions about some of you as well!) Just because you are much thinner and more fit looking I assume you exercise regularly, you always eat healthy and you judge me negatively for my appearance. I do know that my assumptions about you may be just as wrong as what I believe you assumed about me. However, when I see that the larger people in class have placed themselves more to the back of the room, when I have a hard time finding a lab partner and when the lab instructor struggles with how to say to the partner that got stuck with me "things may be different on her", I begin to feel like I am taking something away from the class experience for everyone else. I do not want to hinder another clinician's learning process so I don't push anyone to be my partner, but then I am actually denying myself the learning opportunities I came for. Not to mention that I may be denying the other participants the opportunity to learn how to handle a client that may look and feel like me.
The reality of our world is that there is a very large obese population. I firmly agree this leads to a multitude of chronic illnesses and astronomical medical costs for the individual and our society as a whole. It does need to be addressed on a large scale. However, we as clinicians don’t know where these individuals are on their weight journey. For someone like me who has made drastic lifestyle changes to move me in a positive direction but have not yet gotten my appearance in line with the "norm" that the health care professionals, the media and society are pushing, your response to me can be devastating to my progress, my hope and my desire to continue toward a healthier lifestyle. Again I want to acknowledge that this is as much my problem as it is for those around me and I am addressing this as well. But please have the awareness that an obese person above all is a PERSON FIRST! Then their physical size becomes just another item on the list of "facts" about them, instead of a source of anxiety and separation. Approaching an obese person with respect, acceptance, honesty and openness not only puts them at ease, it also strengthens the rapport that is so crucial in pelvic rehabilitation.
Although I was born and raised in the north east, I now live in Alabama, home of corn bread, fried chicken and sweet tea. The population I deal with is more likely to be at least overweight if not truly obese. So, quite honestly, the practical instruction of how pelvic floor evaluation and treatment may be different with the obese patient would be directly beneficial to my practice. This might include openly addressing in labs how to assess/reposition an obese patient will give each therapist an awareness and confidence when approaching this population and may minimize the patient's embarrassment and keep the doors of trust and communication open. Or taking a moment to recognize the larger participants in the classroom setting and professionally suggesting during a lab session how they can reposition themselves and still affectively achieve appropriate assessment/treatment for the patient would make the transition from class to the reality of the clinic more smooth. Also, taking a moment to offer suggestions for what the obese patient who can’t physically reach their perineum or even palpate the pubic symphysis and or coccyx and doesn’t have a willing partner to assist can do to effectively complete the rehab activities suggested. You have to admit, this is not an easy specialty of practice to broach in the first place, and anything to take the pressure off of the clinician and or patient is helpful!
I so greatly appreciate the respect and professionalism the many delicate topics related to pelvic health are addressed in this program. I would also appreciate that same respect and professionalism when it comes to the reality of the many different body types that are the represented in our practices!"
Thank you to Erin for sharing her thoughtful suggestions, and reminding instructors and fellow course participants that an open, curious and helpful approach is needed for all situations. We at the Institute will address this issue among our instructors so that we can provide more clear guidance regarding patient and provider positioning. Stay tuned for a blog post about helpful positioning and communication tips for working with patients who are obese.
xHerman & Wallace wants to put you in charge of deciding which products we produce! Our philosophy is that we should only be making products which are useful to the therapists who we work with. In our efforts to create products that our registrants find valuable, and keep the price of these products at low as possible, we have been piloting a new product development program. So far this program has seen incredible success, with therapists providing feedback at every step as to how we can make better products for you!
Here is how it works:
1. Herman & Wallace creates a product concept, a description of the product and its contents, without fully creating the product.
2. Herman & Wallace puts this product concept on our website for a trial period. This product concept?s page will contain:
a. A description of the product,
b. the contents of the product (patient forms, powerpoint files, handouts, mapping tools...
c. the estimated retail price of the product,
d. an amount, lower than the retail price, that one can contribute towards this product?s full development called a ?pre-fund? amount,
e. the end date of the trial period.
3. Therapists who would like to buy the product can pre-fund the product concept at a discount to the retail price in exchange for receiving the product upon Herman & Wallace completing its development.
4. Pre-funders will receive an early-release draft of the product and will be asked to provide feedback. Feedback will be solicited for 15 business days following the release of this draft, and comments will be used to make the final version even better.
|
If ten or more therapists pre-fund the product before the end of the trial period, Herman & Wallace will fully develop the product, and will email the product to each therapist who pre-funded the product. |
If less than ten therapists pre-fund the product before the end of the trial period,Herman & Wallace will not fully develop the product, and Herman & Wallace will refund 100% of pre-fund amount paid by each therapist who pre-funded the product. |
To Summarize:
If you see a product you'd like to purchase, pre-fund it and if the product gets 10 or more pre-funders, we'll email you the product after we finish developing it. Pre-funding a product carries NO RISK. If the product does get 10 pre-funders by the end of the trial period, we will refund 100% of the amount contributed by each pre-funder.
All Upcoming Continuing Education Courses








Pelvic Function Level 1 - Satellite - Kankakee IL - May 4 - 5 2024 - SOLD OUT
May 4 2024 - May 5 2024

Pelvic Function Level 1 - Satellite - Ann Arbor MI - May 4 - 5 2024 - SOLD OUT
May 4 2024 - May 5 2024

Pelvic Function Level 2B - Satellite - Fairfax VA - May 11 - 12 2024 SOLD OUT
May 11 2024 - May 12 2024


Trauma Awareness for the Pelvic Therapist - Remote Course - May 11 - 12 2024
May 11 2024 - May 12 2024

Pelvic Function Level 2B - Satellite - East Greenwich RI - May 11 - 12 2024
May 11 2024 - May 12 2024


Sacral Nerve Manual Assessment and Treatment - Remote Course - May 11 - 12 2024
May 11 2024 - May 12 2024


Mobilization of Gastrointestinal Visceral Fascia Satellite Lab Course - Self-Hosted - May 17 - 19 2024
May 17 2024 - May 19 2024

Mobilization of Visceral Fascia: Gastrointestinal Satellite Lab Course - Torrance CA - May 17 - 19 2024
May 17 2024 - May 19 2024

Mobilization of Visceral Fascia: The Gastrointesti System Satellite Lab Course - Bedford NH - May 17 - 19 2024
May 17 2024 - May 19 2024

Mobilization of Visceral Fascia: The Gastrointestinal System - Asheville NC - May 17 - 19 2024
May 17 2024 - May 19 2024

Mobilization of Visceral Fascia: The Gastrointestinal System Satellite Lab Course - Lansing MI - May 17 - 19 2024
May 17 2024 - May 19 2024

Mobilization of Visceral Fascia: The Gastrointestinal System Satellite Lab Course - Scarborough ME - May 17 - 19 2024
May 17 2024 - May 19 2024

Mobilization of Visceral Fascia: Gastrointestinal Satellite Lab Course - Medford OR - May 17 - 19 2024
May 17 2024 - May 19 2024

Pediatrics Level 1 - Treatment of Bowel and Bladder Disorders - Remote Course - May 18 - 19 2024
May 18 2024 - May 19 2024

Pelvic Function Level 1 - Satellite - Phoenix AZ - May 18 - 19 2024 - SOLD OUT
May 18 2024 - May 19 2024

Pelvic Function Level 1 - Satellite - Anaheim CA - May 18 - 19 2024 - SOLD OUT
May 18 2024 - May 19 2024

Pelvic Function Level 1 - Satellite - Oxford AL - May 18 - 19 2024 - SOLD OUT
May 18 2024 - May 19 2024

Pelvic Function Level 1 - Satellite - McKinney TX - May 18 - 19 2024 - SOLD OUT
May 18 2024 - May 19 2024


Mobilization of Visceral Fascia: The Gastrointestinal System Satellite Lab Course - Commerce Township MI - May 17 - 19 2024
May 19 2024 - May 19 2024

Pelvic Function Level 2B - Satellite - Mission Hills CA - May 19 - 20 2024
May 19 2024 - May 20 2024








