
There’s something special about gathering in a room with colleagues, exchanging ideas, practicing hands-on techniques, and learning from expert instructors in real time. While virtual education offers flexibility and accessibility, many pelvic health practitioners are eager to get back to the connection, feedback, and tactile learning that only in-person courses can provide.
If you’re ready to step back into a live classroom, Herman & Wallace has a robust lineup of in-person courses designed to sharpen your clinical skills, deepen your understanding of pelvic health, and connect you with a like-minded community of learners.
Here are some of the in-person courses currently offered:
Pelvic Function Series (In Person)
This progressive pathway is ideal for clinicians looking to build their foundation and then layer on advanced skills.
- Pelvic Function Level 1 – A great entry point into pelvic rehabilitation, this foundational course provides a whole-body framework to assess and treat pelvic floor dysfunction. You’ll gain essential hands-on skills and clinical reasoning strategies.
-
-
- Boston MA - September 6-7
- Detroit MI - November 15-16
- New York NY - December 21-22
-
- Pelvic Function Level 2A, 2B, and 2C – These courses dive deeper into the muscular, fascial, and neurological systems affecting pelvic function. Each level builds upon the previous one, covering complex diagnoses and interventions with plenty of lab time for integration.
-
- Level 2A – Expand your skills in colorectal pelvic health, pudendal neuralgia, and coccyx pain
- Richmond VA - August 9-10
- St. Paul MN - September 13-14
- New York NY - May 31 - June 1
- Level 2B – Expand your skills in pelvic pain, urogynecologic examinations, and treatment options
- Houston TX - June 28-29
- Atlanta GA - September 6-7
- Baltimore MD - September 20-21
- Houston TX - October 4-5
- Richmond VA - November 15-16
- Level 2C – Expand your skills in men’s pelvic health and rehabilitation
- Colorado Springs CO - October 4-5
- Level 2A – Expand your skills in colorectal pelvic health, pudendal neuralgia, and coccyx pain
- Modalities and Pelvic Function – Want to add tools like biofeedback, electrical stimulation, or dry needling to your practice? This course teaches the safe and effective use of modalities within the context of pelvic rehab and pelvic pain.
-
-
- Houston TX - July 12-13
- Akron OH - September 20-21
- Somerset NJ - October 4-5
-
Specialty In-Person Courses
Dry Needling and Pelvic Health Series (In Person) – This hands-on series provides targeted training in the use of dry needling for pelvic conditions.
- Dry Needling and Pelvic Health: Pregnancy – This specialty course explores the safe application of dry needling during pregnancy. Learn how to integrate this modality into perinatal care with a strong emphasis on patient safety, comfort, and outcomes.
-
- Lemont IL - August 23-2
- Dry Needling and Pelvic Health Level 2 – Designed for clinicians who have completed the foundational dry needling course, this course focuses on advanced techniques for addressing pelvic floor and associated neuromusculoskeletal dysfunctions.
Dunluth MN - August 2-3
Pessaries and Pelvic Rehab – Gain hands-on training in assessing, fitting, and managing pessaries for pelvic organ prolapse and incontinence. Learn clinical considerations and practice fitting techniques in supervised labs.
- Chicago IL - November 8-9
- Tacoma WA - January 31 - February 1
High Intensity Perinatal Athletics Practicum –Designed for practitioners working with pregnant and postpartum athletes, this course blends lecture and lab to address clinical decision-making in high-intensity training contexts like CrossFit, HIIT, and Olympic lifting. Understand how to keep your athletic patients safe and strong throughout the perinatal period.
- Somerset NJ - September 27-28
Ready to Join Us In Person?
Whether you’re just starting out or expanding your advanced skills, Herman & Wallace offers a wide range of in-person courses to support your clinical growth. Don’t miss this opportunity to step away from your screen and back into the dynamic environment of hands-on learning.
Explore the full calendar of in-person courses and reserve your spot today. Spaces are limited and tend to fill quickly!

Pamela A. Downey, PT, DPT, WCS, BCB-PMD, PRPC is Senior Faculty with Herman & Wallace and is instructing the upcoming Pudendal Neuralgia and Nerve Entrapment scheduled for January 27, 2024. She is the owner of Partnership in Therapy, a private practice in Coral Gables, Florida where she treats women and men with pelvic floor dysfunction, related urogynecological and colorectal issues, spine dysfunction, osteoporosis, and complaints associated with pregnancy and the postpartum period. Her mission is to educate and integrate healthy lifestyles for patients on the road to wellness. Pam sat down with the Pelvic Rehab to discuss her upcoming course.
What makes pudendal neuralgia such a difficult diagnosis to treat?
I think people often see the content in Pelvic Function Level 1 - Introduction to Pelvic Health and it's like a tidy little box. Then you get the patient and as the practitioner you're like I don't know what to do with this person. We need to show that pudendal skills are needed in differential diagnosis. Even though this course is called Pudendal Neuralgia and Nerve Entrapment, it is about differential diagnosis for a lot of pelvic pain. When you feel more secure in knowing what you're treating and have a systematic way of looking at it, then you can be more productive in your patient care.
I think some ortho therapists treat in a linear fashion, and they go from week one to week eight through a protocol and things generally go well because it's a predictable course when you're rehabbing a total knee replacement, or you have an elbow tendonitis, and you expect these structures to follow a path. But then when you come into the nerve side of things, nerves can be unpredictable. They're influenced by lots of factors. It could be your mood. It could be the range of motion around a joint. It could be a previous history of another neurologic problem feeding it, such as disc pathology. It can be something around a postural habit, and it could be a straight up other dysfunction that then affects the pudendal distribution. And if you don't treat the cause of the initial, you will never improve the latter, which is the neurological presentation in pudendal.
I love that it's more about figuring out the differential diagnosis for pelvic pain and going from that angle into pudendal dysfunction, entrapment, neuralgia, and everything that goes with that. For example, you're going to get a patient with an order for pudendal neuralgia, or even worse entrapment. When they get an order for pudendal neuralgia, then they'll kind of forget that the person may not have pudendal neuralgia. They have problems in the pudendal distribution, but that's basically everything we treat. So as a pelvic rehab practitioner they have to tease it out.
When I look at a script I always say, “that's nice.” The referring doctor may have written it as pudendal neuralgia so that the patient could get reimbursement for the therapy with the diagnosis code. But then we get to add our diagnosis codes on top of that and drive a treatment plan.
So, I think that is a big hangup. Practitioners run when they usually see this diagnosis. You don't want a pudendal patient. Especially if you do not have a lot of skills, because you are going to be like, well, what can I do for this patient? If they sit, they have pain. If they exercise, they have pain. They don't have like a whole repertoire. In the pudendal neuralgia course, we talk about how to figure out if the driver is the spine, the hip, the nerve itself, if it's the pelvic floor musculature, or if it's biomechanical. There are so many facets.
How often do these scripts come in for patients that have pudendal neuralgia?
In pelvic pain they're probably coming in a high percentage, like I would say three-quarters. In practice, depending on who's referring into the person's practice, it's going to be a significant amount of walk-in traffic and referred traffic. Because every levator syndrome patient could have a pudendal issue driving the levators, and long-standing levator pain can end up being pudendal.
It's kind of like are you treating the chicken or the egg? I think giving the person skills to do test and retest and having a way to keep falling back on to this and then to also be able to transmit the idea that this isn't a fix -it problem. You know, we just don't put a band aid on it and you're done. Other folks who are more newish, who expect this linear event, they're going to struggle because there's going to be setbacks and sometimes doing more is the exact opposite of what needs to be done. Less is more.
When you look at the H&W course catalog, where would you recommend that practitioners take the Pudendal Neuralgia course?
The sweet spot for taking the pudendal neuralgia course would be practitioners who have taken PF1 and Pelvic Function Level 2A - Colorectal Pelvic Health, Pudendal Neuralgia, and Coccyx Pain, because they learn the rectal canal and PF2A. Practitioners who focus specifically on treating the male pelvic patient would benefit from this course because it is a good thinking course for how to treat men. It could pair well with Pelvic Function Level 2C - Men’s Pelvic Health and Rehabilitation (formerly Male Pelvic Floor). In my practice I get a lot of men coming in because they look on the internet and decide that they got pudenda neuralgia.
If you understand differential diagnosis you can touch on is this a sciatic nerve problem? Is this a genitofemoral problem? We look at the lumbo-sacral plexus in a decision tree, and then we then focus on pudendal and then how people manage them from a medical standpoint and from a therapy standpoint. I talk about using a rule-out method - this could be genital femoral, this could be pudendal nerve. And then you prove what the problem is by doing test and retest.
There's also a lot of pain neuroscience, so practitioners who have taken Pain Science for the Chronic Pelvic Pain Population would benefit from this course. The pudendal neuralgia course goes really well with this course because the practitioners who have taken the pain science course already know that there's going to be ups and downs. Also Nari Clemon’s nerve courses, Lumbar Nerve Manual Assessment and Treatment and Sacral Nerve Manual Assessment and Treatment, are definitely lab -oriented courses and this could be a backgrounder even going into her series, because she's going to talk about a lot of nerve techniques that can be then applied to the pudendal. Nari's courses give solid hands-on skills to deal with nerves, palpation, and finding them. Then this course shows you how to treat them. Not necessarily Pudendal, but all the nerve things. These courses enhance each other. It's like a decision tree where pudendal is on there and you can pass through it and go into Nari’s stuff where you can get a good idea and then use your myofascial, your orthopedic, your neuro skills.

We are pleased to announce the following changes and additions to our core series of courses. These changes are being undertaken by our Curriculum Development Team based on evolving realities of our field and the body of evidence and literature. In keeping with the way the field has evolved, we will be making the following changes to our core coursework.
Two courses will be joining our Pelvic Function Series:
- Pelvic Function Modalities - This brand new course is an in-person two-day continuing education course targeted to pelvic health clinicians covering frequently used modalities in pelvic health, including biofeedback and EStim. Hands-on labs using a variety of equipment necessitate that this course be offered in-person, where participants can practice using the equipment.
- Pelvic Function Level 2C: the Male Pelvic Floor and Men’s Pelvic Health - formerly the stand-alone course, Male Pelvic Floor Function Dysfunction and Treatment, this course is now being adapted and reformatted to be a part of the Pelvic Floor Series, reflecting the inclusive stance of H&W core series instructing in the care of all patients. This course will be offered as satellite, self-hosted, and in-person options in order to provide the most flexible pathway for participants.
In addition to these two new offerings, you will see greater inclusion of all genders throughout the series, starting with PF1. The modified titles and topics will be as follows:
Pelvic Function Level 1: Introduction to Pelvic Health - this course will provide a thorough and comprehensive introduction to anatomy and physiology of the pelvis and surrounding structures in all genders. Includes an introduction to performing intra-vaginal exam. This course will be offered in satellite and in-person formats.
Pelvic Function Level 2A: Colorectal Pelvic Health and Pudendal Neuralgia, Coccyx Pain. In labs, anorectal internal exam will be introduced. This course will be offered in satellite and in-person formats.
Pelvic Function Level 2B - Urogynecologic Topics in Pelvic Health. This course will be offered in satellite, self-hosted and in-person formats
Pelvic Function Series Capstone - Integration of Advanced Concepts in Pelvic Health. This course will remain targeted to the advanced clinician. A greater emphasis on workshopping clinical case studies will be incorporated. This course will be offered in satellite, self-hosted and in-person formats.
Questions:
What courses will be required in order to advance to the Capstone course?
As we understand the “advanced pelvic floor clinician” may have a variance of experience and focuses, the following course “journeys” can all be taken in order to take the Capstone course:
PF1
PF2A
P2B and/or PF2C
The Modalities course is strongly recommended, but not required, in order to take the Capstone course.
Why is the series being expanded and updated in this way? .
It is a reality of our field that pelvic rehab evolved from a tradition of “women’s health physical therapy”, and that is reflected in the vulvovaginal emphasis of the current coursework. As the scope of pelvic rehab has expanded to encompass men’s health and care for all genders, it is important that all pelvises be incorporated at every level of our series, and that men’s health be a foundational part of our curricula, rather than being siloed as a specialty offering.
I have already started my PF series coursework, where do I go now?
If you have taken only PF1, you should advance to PF2A, 2B or 2C in any order. You may also wish to take the Modalities course in order to learn evidence-based use of modalities and practice biofeedback and Estim in a hands-on, in-person setting. The best way to choose which course to take next will be determined by who shows up in your clinic after completing PF1 and beginning to see your first pelvic patient caseload.
If you have taken PF1 and 2A - take either 2B or 2C or both in any order to advance to Capstone. If you took PF1 following the pivot to the satellite model, you may also wish to take the Modalities course in order to practice hands-on biofeedback and Estim labs.
If you have taken PF1 and 2B, you must take 2A prior to Capstone. You may take the 2C course to learn men’s health topics if seeing male and male-identifying patients is part of your clinical goals. If you took PF1 following the pivot to the satellite model, you may also wish to take the Modalities course in order to practice hands-on biofeedback and Estim labs
If I have taken PF1, 2A, and 2B - you may advance to Capstone or you may take the 2C course to learn men’s health topics if seeing male and male-identifying patients is part of your clinical goals. If you took PF1 following the pivot to the satellite model, you may also wish to take the Modalities course in order to practice hands-on biofeedback and Estim labs
If you have taken PF1, 2A, 2B and Capstone but have not taken the former Male Pelvic Floor course, you may take the 2C course to learn men’s health topics if seeing male and male-identifying patients is part of your clinical goals.
If you have taken PF1, 2A and the Male Pelvic Floor course, you may advance to Capstone
If you have taken PF1, 2A, 2B and the Male Pelvic Floor course, you may advance to Capstone
Am I required to take more courses in order to complete the PF series now?
No. Previously, there were three prerequisite courses for taking the advanced Capstone course: PF1, 2A and 2B. Following the changes to the series, the prerequisite courses for taking Capstone will be PF1, 2A and 2B OR 2C (or both, depending on one’s target patient population). The Modalities course is a strongly encouraged, but not required, level of the PF series.
As before, participants should choose their next course based on the patient needs they are seeing in the clinic. Following PF1, many may see patients with fecal incontinence or coccyx pain and may choose to prioritize PF2A as the next step in their journey. Others may see patients with penile pain or incontinence post-prostatectomy and may choose to take 2C as their next step.
As before, there are no required courses in order to sit for the Pelvic Rehab Practitioner Certification Exam.
Why aren’t there self-hosted options for PF1 and PF2A?
PF1 is most learners’ first introduction to performing intra-vaginal assessment and therefore we believe the best learning experience will be under the guidance of either an HW faculty member or trained teaching assistant at an in-person or satellite course. Similarly, PF2A is most learners’ first experience performing anorectal exam, which should also take place under the supervision of an experienced clinician. In PF2B, 2C, and Capstone, these techniques are refined and it is therefore appropriate to allow self-hosted options for those who have already learned these skills and are comfortable with independent learning.
I see that there will be options for a few in-person as well as satellite offerings for much of the series. Will HW continue to offer both formats?
We understand that many people appreciate the flexibility and accessibility of the satellite model as an improvement over the days when all series courses were sold out with long waitlists and lengthy travel was often required to attend our courses. We also understand that some folks simply prefer the format in which instructors are present at the course. Our intention is to offer formats that accommodate everyone’s needs, which is why the PF series will be available in-person as well as in the satellite format starting in 2024. Because of the hands-on equipment needs of the Modalities course, this will be available exclusively in person.
Why is PF1 required for 2C if it wasn't for MPF?
Historically, the Male Pelvic Floor course was a stand-alone course, meaning that many participants would take this course after beginning their journey with PF1 and after already seeing patients with pelvic floor dysfunction. Others, often male and male-identifying practitioners who did not feel their goals were met by the vulvovaginal-centered PF series, would take the Male course as their first ever introduction to pelvic health. This resulted in course attendees being in vastly different places in terms of experience, which often results in a sub-optimal learning experience for all.
As part of our push to see more information about patients of all genders incorporated at every level of the core series, PF1 which contains foundational information on all pelvises and core concepts in pelvic rehab, will be a prerequisite for 2C, which will build on those core concepts as they apply specifically to the male and male-identifying patient.
Who can act as a Teaching Assistant for the series courses in the new format?
PF1 - must have PF1, and ⅔ of the Level 2s (2A, 2B, and 2C)
PF2A - must have 1, 2A, and 2B or C
PF2B - must have 1, 2B
PF2C - must have 1 and have taken the Male Pelvic Floor in 2016 or later
Capstone - must have 1, 2A, 2B or 2C, and Capstone

Kate Bailey, PT, DPT, MS, E-RYT 500, YACEP, Y4C, CPI joins the Herman & Wallace faculty with her new course on Restorative Yoga for Physical Therapists, which is launching in remote format this June 6-7, 2020. Kate brings over 15 years of teaching movement experience to her physical therapy practice with specialities in Pilates and yoga with a focus on alignment and embodiment. Kate’s pilates background was unusual as it followed a multi-lineage price apprenticeship model that included study of complementary movement methodologies such as the Franklin Method, Feldenkrais and Gyrotonics®. Building on her Pilates teaching experience, Kate began an in depth study of yoga, training with renown teachers of the vinyasa and Iyengar traditions. She held a private practice teaching movement prior to transitioning into physical therapy and relocating to Seattle.
 Yoga is a common term in our current society. We can find it in a variety of settings from dedicated studios, gyms, inside corporations, online, on Zoom, at home, and on retreat. The basic structure of a typical yoga class is a number of flowing or non flowing postures, some requiring balance, some requiring going upside down, and many requiring significant mobility to achieve a certain shape. At the end of these classes is a pose called savasana, corpse pose (or sometimes translated for comfort as final resting pose). In this pose, which is often a treat for students after working through class, students lie on the ground, eyes closed, possibly supported by props, and rest. It is perhaps the only other time in the day when that person is instructed to lie on the floor in between sleep cycles.
Yoga is a common term in our current society. We can find it in a variety of settings from dedicated studios, gyms, inside corporations, online, on Zoom, at home, and on retreat. The basic structure of a typical yoga class is a number of flowing or non flowing postures, some requiring balance, some requiring going upside down, and many requiring significant mobility to achieve a certain shape. At the end of these classes is a pose called savasana, corpse pose (or sometimes translated for comfort as final resting pose). In this pose, which is often a treat for students after working through class, students lie on the ground, eyes closed, possibly supported by props, and rest. It is perhaps the only other time in the day when that person is instructed to lie on the floor in between sleep cycles.
Savasana is one of many restorative yoga postures. In the work created and popularized by Judith Hanson Lasater, PT, PhD1, restorative yoga has taken a turn away from the active physical postures, breath manipulations and meditations that are commonplace in how we think of yoga. She has focused on rest and the need for rest in our current climate of productivity, poor self-care, and difficulty managing stress and pain.
In a dedicated restorative yoga class (not a fusion of exercise then rest, or stretch then rest… which are really lovely and have their own benefits), a student comes to class, gathers a number of props, and is instructed through 3 to 5 postures, all held for long durations to complete an hour or longer class. Consider what it would look like to do 3 things over one hour with the intent of resting. It is quite counter-culture. Students have various experiences to this type of practice, but overtime many begin to feel the need for rest (or restorative practice) in a similar way that one feels thirsty or hungry.
We know the benefits of rest: being able to access the ventral vagal aspect of the parasympathetic nervous system is what Dr. Stephen Porges2 suggests supports health, growth and restoration. There is impact on the ventral vagal complex in the brainstem that regulates the heart, the muscles of the face and head, as well as the tone of the airway. To heal, we need access this pathway. To manage stress, we need to access this pathway. To be able to choose our actions rather than be reactionary, we need to access this pathway. Restorative yoga is an accessible method that may be a new tool in a patient’s tool box to help manage their nervous systems.
1. Relax and Renew: Restful Yoga for Stressful Times by Judith Hanson Lasater PT, PhD
2. Polyvagal Theory by Stephen W Porges PhD

Herman & Wallace is excited to announce an upcoming course on pelvic rehab for the gender diverse patient, written and instructed by Dr. Laura Meihofer, DPT, ATC. As Dr. Meihofer indicated in a recent blog, "[t]he number of individuals who identify as transgender is growing each year. The Williams Institute estimated in 2016 that 0.6% of the U.S. population or roughly 1.4 million people identified as transgender (Flores, 2016)... With the rise of individuals who identify as transgender, gender non-binary and intersex, healthcare professionals have equally seen an influx of patients who require care throughout their discovery and transition."
The new course from Dr. Meihofer is called "Gender Diversity and Pelvic Health: Comprehensive Care for Transgender Men and Women", and it will be debuting on May 29-31, 2020 in Livingston, NJ.
Dr. Meihofer was kind enough to share some thoughts about the new course, her practice, and herself with The Pelvic Rehab Report. Thank you, Laura!
Tell us about yourself, Laura!
My name is Laura Meihofer and I’ve been a physical therapist for 7 years. I work at Mayo Clinic and I see patients throughout the gender spectrum who most commonly struggle with pelvic floor dysfunctions relating to overactive muscles such as: chronic and acute pelvic pain, urinary frequency/urgency/incontinence/hesitancy, constipation, pain with intercourse, low back and hip pain.
 What can you tell us about your new course, "Gender Diversity and Pelvic Health"?
What can you tell us about your new course, "Gender Diversity and Pelvic Health"?
Currently there are roughly 1.25 million transgender identified individuals in the United States and this number is growing. This course will help to dispel the idea of “other” when treating this demographic and demonstrate how much sameness there is when treating pelvic floor dysfunction.
These skills will greatly benefit any practice as this population is so underserved, they are looking for allies that are not just nice but competent. When you are able to successfully treat gender diverse patients, they spread the word about the great care they received and you now have a strong referral base. Taking this course opens up a whole new referral base of amazing people.
This course will not only feature videos from thought leaders in the field but will also highlight testimonials from patients and caregivers who have undergone their own gender transitions.
What essential skills does your course add to a practitioner’s toolkit?
I think the most important technique that attendees will learn will be how to assess a trans women and trans man after they have undergoing genital reconstruction surgery. Attendees will gain competence in the care of the gender diverse patient at any stage during their gender transition.
What was your inspiration to create this course for trans-identified patients?
Working at a major medical institution, I found that it was difficult finding providers in a patient’s area that were competent in care of a transgender patient. As I talked more and more with various physical therapists I realized they were thirsty for knowledge on how to serve these individuals. So I created the course!
What prepared you to create this course?
The most important thing I have done for this course is treat hundreds of patients who are trans identified throughout their gender journey. This allowed me to not only see all the medical interventions they went through but also to hear their personal journey of transition. These experiences expanded my empathy for what they go through and inspired me to search within myself on how I can be better for them. This desire to improve opened a creative well inside of me from which this course grew.
Discuss the effect conditions covered in your course have on a patient’s quality of life, your experience treating patients with this condition, and how their quality of life has increase after successful treatment.
Individuals who identify as transgender suffer from pelvic floor dysfunction just like our cis gender folks. There is no current data to capture the prevalence of pelvic floor issues in this specific population to date, however there is research to support the overall lack of care these individuals receive. Based on the results from the U.S. Transgender Survey which surveyed 28,000 respondents, the numbers in the health care field were staggering.
33% of respondents had at LEAST one negative experience with a health care provider in the last year due to being transgender. Negative experiences were qualified as verbal harassment, refusal of treatment or having to teach the health care provider about transgender people to receive appropriate care. 23% of respondents did not see a doctor when they needed to due to fear of being mistreated as a transgender person.
This course aims has two primary aims:
1) Educate providers on the unique concerns that transgender individuals experience related to hormone replacement and surgical techniques.
2) Equip attendees to provide competent care for this demographic
Join Dr. Meihofer for Gender Diversity and Pelvic Health this May 29-31, 2020 in Livingston, NJ!
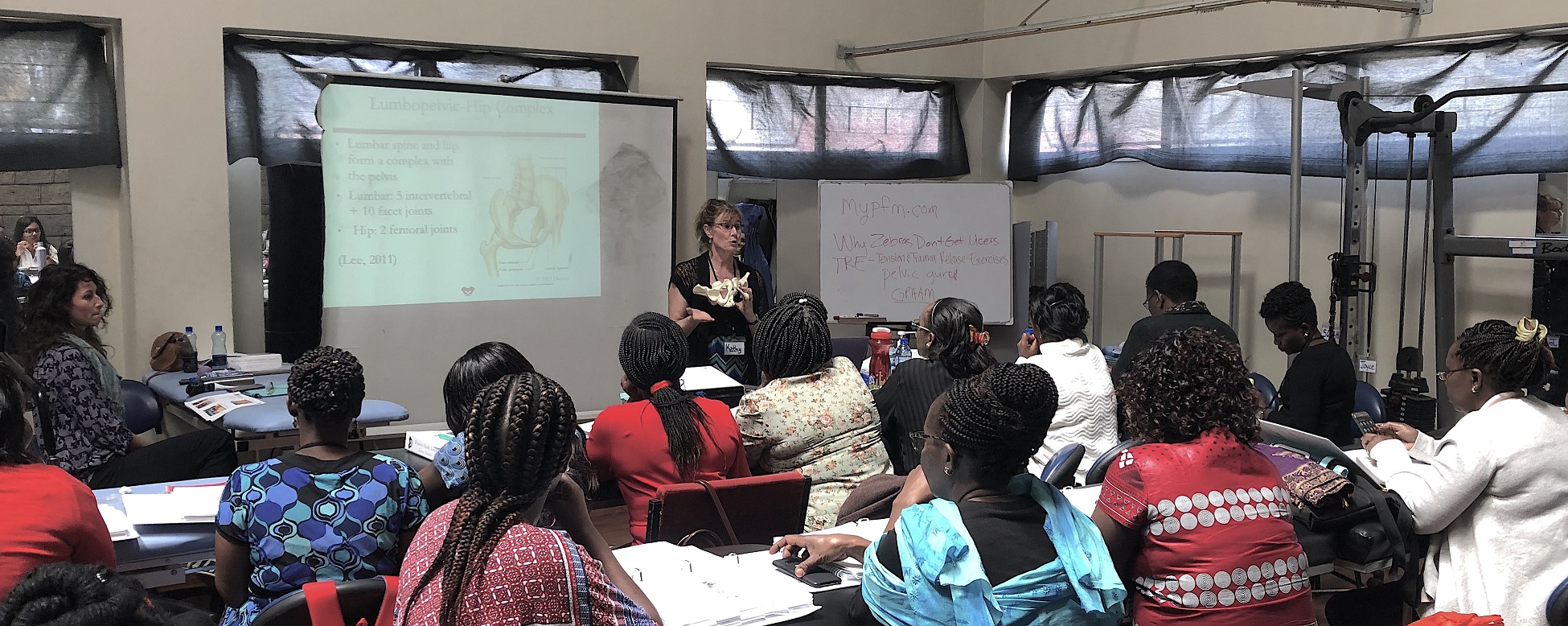
Earlier this year, Herman & Wallace sponsored the first ever pelvic rehab course for physios in Nairobi, Kenya in partnership with The Jackson Clinics Foundation. After returning from that course, Kathy Golic, PT spent months writing a new course, adapting information from Pelvic Floor Level 1, Level 2A, and the Pregnancy and Postpartum series. This October, Kathy (along with co-instructors Casie Danenhauer and Sherine Aubert) returned to teach her follow-up course that expanded on the first module, introducing lectures and labs tailored to the community of pelvic physios in Kenya. This dispatch comes from instructor Kathy Golic, PT, who sent in this article shortly after returning from the course. Huge thanks to Kathy and her colleagues Sherine Aubert and Casie Danenhauer for doing this important work!
 It has been a week now, and as I type looking out on the windy rainy day, it is hard to believe that I was so recently in a warm, sheltered classroom sequestered from the hustle and bustle of Nairobi. A place which has captured my heart. Really it is the people, especially my new “sisters” who I spent so much time with during this last two-week course module. Once again, I experienced chill bumps every day from witnessing the growth, the stories, the wisdom and the compassion of these bright, motivated, committed physiotherapists who came back for the 2nd module in our series to help them become experts in the field of Pelvic Health. This module covered topics of Pregnancy, Postpartum care, Prolapse, Colorectal Conditions including fecal incontinence and constipation, and Coccydynia. We had a terrific printed course manual for this 2nd in the series, thanks to the partnership of Herman and Wallace and Jackson Clinics Foundation. With my wonderful and resourceful, skilled colleagues from LA, Casie Danenhaur, and Sherine Aubert, we included comprehensive lectures, lively demonstrations, hands on creative experiential learning opportunities, and awesome supervised lab training sessions. We also had a lot of case study discussions, and live case studies where we assisted the students, who are practicing physiotherapists, in conducting thorough assessments and clinical reasoning processes to treat and make plans to further the progress of their patients.
It has been a week now, and as I type looking out on the windy rainy day, it is hard to believe that I was so recently in a warm, sheltered classroom sequestered from the hustle and bustle of Nairobi. A place which has captured my heart. Really it is the people, especially my new “sisters” who I spent so much time with during this last two-week course module. Once again, I experienced chill bumps every day from witnessing the growth, the stories, the wisdom and the compassion of these bright, motivated, committed physiotherapists who came back for the 2nd module in our series to help them become experts in the field of Pelvic Health. This module covered topics of Pregnancy, Postpartum care, Prolapse, Colorectal Conditions including fecal incontinence and constipation, and Coccydynia. We had a terrific printed course manual for this 2nd in the series, thanks to the partnership of Herman and Wallace and Jackson Clinics Foundation. With my wonderful and resourceful, skilled colleagues from LA, Casie Danenhaur, and Sherine Aubert, we included comprehensive lectures, lively demonstrations, hands on creative experiential learning opportunities, and awesome supervised lab training sessions. We also had a lot of case study discussions, and live case studies where we assisted the students, who are practicing physiotherapists, in conducting thorough assessments and clinical reasoning processes to treat and make plans to further the progress of their patients.
 All of this in itself was incredibly rewarding. But there was more. The power of sacrifice we witnessed. The power of solidarity and true generosity. Most of these women continued to have to work after class even while in this two-week module; in class from 8-4, but then going on their way, some of them through heavy Nairobi traffic, to treat patients in their offices, or to work hospital shifts. One student heading out after a Wed. afternoon class told me that she was going to work from 7- midnight, then would sleep until 4am, then back to work until 7 am, before returning to class at 8 am. She also had to miss one class to participate in her mentorship for her ortho advanced diploma, so had to make up a test with us the next day. (she aced the test!) Now for the generosity. I will share just 1 of many stories. One of the physios asked a patient of hers whom she felt she could use some help with, if she would mind traveling to the KMTC classroom where we were teaching so the other students could learn, while we the visiting instructors, would help guide in her assessment and care. This woman agreed, and got up at 3:30 am, traveled by bus for 3 hours to come for her treatment. She willingly shared her story, and it was tough to hear. She worked as a vegetable vendor carrying produce on her back, lifting it, and sitting on a stone for hours each day. She, a mother of 5 grown children with an unemployed husband. Her physio and the class did quite well in their assessment and with treatment and suggestions. She seemed pleased. Then as she prepared to leave, some of the physio students “passed the hat” and collected 7,000 kshillings (about $70.00) and presented this humble lady with the money so that she could afford transportation home. It is my understanding that most Kenyans spend 50% of their income on food, so sharing with this patient was a true sacrifice. But for these ladies, there was no question about it. This is how they live and how they work. They are themselves so grateful for the knowledge, skills and experience that they are getting through this program, and they will pay it backwards and forwards. My colleagues this time and last time, are also indebted to them for all they have taught us. It is truly an honor and privilege to be part of this great program, and I too am thankful for all the team players in this venture.
All of this in itself was incredibly rewarding. But there was more. The power of sacrifice we witnessed. The power of solidarity and true generosity. Most of these women continued to have to work after class even while in this two-week module; in class from 8-4, but then going on their way, some of them through heavy Nairobi traffic, to treat patients in their offices, or to work hospital shifts. One student heading out after a Wed. afternoon class told me that she was going to work from 7- midnight, then would sleep until 4am, then back to work until 7 am, before returning to class at 8 am. She also had to miss one class to participate in her mentorship for her ortho advanced diploma, so had to make up a test with us the next day. (she aced the test!) Now for the generosity. I will share just 1 of many stories. One of the physios asked a patient of hers whom she felt she could use some help with, if she would mind traveling to the KMTC classroom where we were teaching so the other students could learn, while we the visiting instructors, would help guide in her assessment and care. This woman agreed, and got up at 3:30 am, traveled by bus for 3 hours to come for her treatment. She willingly shared her story, and it was tough to hear. She worked as a vegetable vendor carrying produce on her back, lifting it, and sitting on a stone for hours each day. She, a mother of 5 grown children with an unemployed husband. Her physio and the class did quite well in their assessment and with treatment and suggestions. She seemed pleased. Then as she prepared to leave, some of the physio students “passed the hat” and collected 7,000 kshillings (about $70.00) and presented this humble lady with the money so that she could afford transportation home. It is my understanding that most Kenyans spend 50% of their income on food, so sharing with this patient was a true sacrifice. But for these ladies, there was no question about it. This is how they live and how they work. They are themselves so grateful for the knowledge, skills and experience that they are getting through this program, and they will pay it backwards and forwards. My colleagues this time and last time, are also indebted to them for all they have taught us. It is truly an honor and privilege to be part of this great program, and I too am thankful for all the team players in this venture.


Aparna Rajagopal, PT, MHS is the lead therapist at Henry Ford Macomb Hospital's pelvic dysfunction program, where she treats pelvic rehab patients and consults with the sports therapy team. Her interests in treating peripartum patients and athletes allowed her to recognize the role that breathing plays in pelvic dysfunction. She has just joined the Herman & Wallace faculty and co-authored the new course, "Breathing and the Diaphragm: Pelvic and Orthopedic Therapists", which helps clinicians understand breathing mechanics and their relationship to the pelvic floor.
Aparna was kind enough to introduce herself to us here on The Pelvic Rehab Report.
 Thank you for your time Aparna! To start, tell us a little bit about yourself.
Thank you for your time Aparna! To start, tell us a little bit about yourself.
My name is Aparna. I’ve been a physical therapist for 22 years. About 16 years ago I switched focus from orthopedics to treating pregnancy and postpartum patients and that’s where my initial interest in pelvic care started. In 2006 following my pregnancy and birth of my daughter, my interest in pelvic care grew with my special interest becoming pelvic pain.
I teach and mentor the pelvic health therapists within the fairly large hospital system that I work at and collaborate with our spine center team and our sports team.
What can you tell us about this new breathing course that is not mentioned in the “course description” and “objectives” that are posted online?
Physical therapy has evolved and continues to evolve as we speak. Regional inter dependence, wherein the different systems interplay, and one structure influences another, is fascinating. No longer is the body considered and treated as independent fragmented pieces. The ‘core’ with the contribution of the Diaphragm and the pelvic floor is so much more than just the Transverse Abdominis and the Multifidus working together. Fascial restrictions of the lower abdomen and the pelvis can influence how the low back feels, thoracic stiffness can influence the interplay between the various abdominal muscles by way on their insertion into the lower ribs, musculo- skeletal pain and postural deviations can stem from incorrect breathing patterns etc.
Normal breathing rate is about 10 times every minute. Breathing incorrectly reinforces wrong movement patterns tens of thousand times a day with negative consequences on the musculoskeletal system.
This course offers an in depth look at the diaphragm from the perspective of both orthopedic and pelvic therapists and attempts to tie in the diaphragm to the thoracic spine, the ribs, the pelvic floor, the core, posture and finally the athlete.
What essential skills does the breath course add to a practitioner’s toolkit?
The practitioner will walk away with the ability to view the patient as a “whole”. It offers a different perspective on neck and back pain, posture/ alignment along with the ability to assess for and connect breathing and the diaphragm to stability/ the core, continence issues and the Autonomic Nervous System.
As therapists we already do a great job of addressing strength issues, assessing and correcting posture, mobilizing etc. You can add to your treatment options by learning how the diaphragm works in concert with other muscles (especially the abdominals) and systems, identifying breathing pattern dysfunctions and postures, and movement patterns which may be linked to breathing pattern dysfunctions. This understanding is beneficial for both orthopedic and pelvic patients.
What inspired you to create this course? What void does this new offering fill?
I have used breathing and evaluation of the diaphragm as a part of pelvic care for several years now. As the mentor for the pelvic program at my hospital, and as a part of the spine team and sports team, I work with pelvic therapists, orthopedic therapists, manual certified therapists, and sports certified therapists. Through my interactions I have come to realize that although many of the therapists are aware that the Diaphragm and breathing are important, they are unsure of how to assess for dysfunctions and address those dysfunctions. I initially started conducting classes within the hospital system. At the same time Leeann who is a sports certified therapist and holds a manual therapy certificate and I started collaborating on our patients. Using a combination of her knowledge and effective manual techniques with my pelvic care and breathing techniques we realized that along with my pelvic patients; our back and neck patients, and her sports patients were all benefitting from this combined approach. We realized along the way that we had information worth sharing with our colleagues that would benefit them in treating their patients, and started classes within the hospital system and that is how this class was born!
What was your process like creating this course?
As a trained pelvic therapist, I have incorporated and used breath and the diaphragm in my treatment for over a decade. Leeann and I have created this course using a combination of our clinical experiences, our education in our respective chosen paths of patient care, and most importantly using recent and relevant research articles from journals to guide us extensively in creating this course.
Breathing and the Diaphragm: Pelvic and Orthopedic Therapists is a new course being offered next March 27-29, 2020 in Sterling Heights, MI, and again on December 11-13, 2020 in Princeton, NJ. It is created and taught by Aparna Rajagopal, PT, MHS and Leeann Taptich, PT, DPT. Come learn how the diaphragm and breathing can affect core and postural stability through intra-abdominal pressure changes. As an integrated approach, the course looks at structures from the glottis and the cervical region to the pelvic floor and helps in understanding a multi component system that works together.

As more and more patients seek care for pelvic floor dysfunction, the need for more qualified practitioners is becoming apparent. Many patients prefer to see a clinician who they identify with, which is why it is important for practitioners of all genders to learn to treat pelvic floor dysfunction. Because much of the public's awareness of pelvic rehab comes out of women's health, the vast majority of pelvic health practitioners are women.
There is currently a shortage of male pelvic health practitioners. To help us understand why it is so important to fix that, we reached out to several male clinicians who have attended the Male Pelvic Floor: Function, Dysfunction, and Treatment course to ask them about the need for more men in the field. Here are some answers to the question:
“Why is it important to have male providers available to treat male patients in the field of pelvic health?”
Grant Headley of Bridgetown Physical Therapy of Portland, Oregon (www.bridgetownpt.com)
While as PT’s we all approach our patients with interest in helping them as individuals, some of our patients feel more comfortable sharing certain details with a provider of the same gender. Many of the hang-ups some men have about receiving care from a female provider are related to an older generation, to certain traditional or religious cultural beliefs, or to certain beliefs about propriety related to receiving care.
As acknowledged in our coursework, generally men have cultural barriers that traditionally do not permit sharing of vulnerability or weakness, especially in the sexual domain. Here are a few unsolicited statements I feel encapsulate what my own male patients have told me: Some heterosexual men feel more comfortable sharing the details of their dysfunction with a man because they find it difficult to admit vulnerability in the presence of a female. Some men prefer not to relay the clinically pertinent details of dysfunctional sexual encounters with a female because they do not wish to make the female practitioner uncomfortable. Many men feel that they can relay more detail about the mechanics of the sexual dysfunction or signs of improvement to a male provider. Some men have told me that they felt their sexual dysfunction was minimized or that they have been treated with patronizing language by a female pelvic PT in the past. Unfortunately, these patients attribute this negative experience to the PT being female, and they are not comfortable having a second opinion with a female.
 Although we strive to present as open-minded and neutral to our patients, they may have an affinity for a male provider. This could foster a more constructive clinical partnership towards working on their goals if they perceive fewer communication barriers. I can offer my own experience as a past patient suffering with pelvic floor dysfunction; I was so desperate for help and I felt so grateful that there was a physical therapist in my city at all that was willing to help me. I did not care that she was female and that I had to receive treatment at a women's health clinic for new mothers in the University Hospital. Many female therapists reading this article have likely transferred lifesaving PT care to scores of men. This organization of H&W that does so much good for a sensitive aspect of men's care is dominated by women- this needs to be acknowledged as a net positive but also appreciated that much of the education and application of care is an adaptation from what has worked for women in the past. Many men will be so grateful to receive care and get better. Some men unfortunately will have barriers to receiving care and for those patients, we can seek out and encourage our male colleagues to get involved in pelvic rehab so we can all provide more access to care.
Although we strive to present as open-minded and neutral to our patients, they may have an affinity for a male provider. This could foster a more constructive clinical partnership towards working on their goals if they perceive fewer communication barriers. I can offer my own experience as a past patient suffering with pelvic floor dysfunction; I was so desperate for help and I felt so grateful that there was a physical therapist in my city at all that was willing to help me. I did not care that she was female and that I had to receive treatment at a women's health clinic for new mothers in the University Hospital. Many female therapists reading this article have likely transferred lifesaving PT care to scores of men. This organization of H&W that does so much good for a sensitive aspect of men's care is dominated by women- this needs to be acknowledged as a net positive but also appreciated that much of the education and application of care is an adaptation from what has worked for women in the past. Many men will be so grateful to receive care and get better. Some men unfortunately will have barriers to receiving care and for those patients, we can seek out and encourage our male colleagues to get involved in pelvic rehab so we can all provide more access to care.
Lance Frank of Flex Physical Therapy in Atlanta (www.flexptatl.com)
Personally, as a male provider in pelvic health, I find that the men I treat are much more comfortable and at ease discussing topics like erections (or lack thereof) and sexual dysfunction, as well as incontinence, or pelvic pain. In a female dominated sub-specialty of physical therapy, sometimes as a male it can be intimidating and even embarrassing for some men to discuss these topics at all, let alone with a female; so having the option to speak and be treated by another male who may better understand the changes, anatomy, and problems they’re experiencing may feel a bit less daunting. Our culture has made male masculinity fragile and I think some populations of men who need pelvic floor rehab may feel embarrassed to be treated by a female clinician if their perception of being seen by a female is emasculating. Ultimately, I think there needs to be more men in this field because there needs to be better visibility of male pelvic health providers in general, as well as better representation of men acknowledging that male pelvic floor disorders exist and are willing and able to treat them.
Eddie Gordon of Flow Rehab in Seattle (www.flowrehab.com)
There are far fewer male physiotherapists treating men with pelvic floor dysfunctions, but I am hopeful this will change for the better. Lack of access to male pelvic physios is a relative barrier to care because some men are more comfortable seeing a male pelvic provider the same way most women would prefer seeing a female pelvic physio. In general, men do not typically seek treatment as frequently or early enough the way most women do. If male pelvic physios are not available, then men may more likely delay treatment, which could potentially worsen their problem. Ironically, when it comes to men with pelvic floor dysfunctions, men are underrepresented, but I am hopeful that more male PT’s will be joining the movement to educate the male population.
Milan Patel of Comprehensive Therapy Services in San Diego (comprehensivetherapy.com)
I believe it's important to have male providers in the pelvic health field for many reasons, one being the opportunity for connection. I think we connect best with reflections of ourselves and for men seeking out a pelvic health provider that can be hard to find. In my experience, pelvic physical therapy works best when your patient can be open and honest, and establishing a strong connection between therapist and patient is the first step. Another reason is that people should have options for the provider they want. In San Diego I am the only male pelvic physical therapy provider which means most men seeking pelvic floor therapy have no choice but to see a female. If you switched the genders in the last sentence you could see how that is problematic. Many women prefer to have their pelvic PT be a female, I just think guys should get the same choice.
Steven Lavender of The Physical Therapy Practice NYC in New York (thephysicaltherapypractice.nyc)
In my experience as a gay male practitioner practicing pelvic floor physio on only men:
Gay male patients usually prefer a gay provider because they feel like they don’t have to explain lifestyle issues and choices, they may be unused to being touched by women, and maybe misogynistic.
Some straight men have told me that they think a male practitioner would know more about their pelvic issues than a woman. Some men don’t think women are strong enough nor have long enough fingers to get to the places they need to be. Some straight men report they might be attracted to a female therapist and get an erection or feel embarrassed about appearing unmanly with their particular pelvic condition.
For some men being touched by a woman is a religious issue so many males of the Jewish and Muslim faiths prefer to see a male practitioner.
Some men could not care less who sees them as long as they get better.
One woman called me for advice or for an appointment from some distance because they "figured a gay man in New York City just might know more about my ass and ass pain than any local jack-assed doctor in my neck of the woods." True story.
If you are interested in learning to treat male patients, the Male Pelvic Floor: Function, Dysfunction, and Treatment course is a great place to start! The course is taking place twice more in 2019, this September 13-15, 2019 in Pasadena, CA, and again in Fort Myers, FL on October 19-21, 2019. We are already booked four times in 2020 as well, so be sure to check out the full course schedule for all available dates.


The number of individuals who identify as transgender is growing each year. The Williams Institute estimated in 2016 that 0.6% of the U.S. population or roughly 1.4 million people identified as transgender (Flores, 2016). This was a 50% increase from a 2011 survey which estimated only 0.3% or 700,000 people identified as transgender (Gates, 2011). Though these numbers are growing each year, due to increased visibility and social acceptance, it is presumed that these numbers are underreported due to inadequate survey methods, stigma/fear associated with “coming out” and deficient definitions of the multitude of options for gender identity (Flores, 2016).
![]() With the rise of individuals who identify as transgender, gender non-binary and intersex, healthcare professionals have equally seen an influx of patients who require care throughout their discovery and transition. Though medical intervention for these individuals is not new, the first documented surgery was in 1922 to Dora Richter, it has often been segmented and lacking in evidence-based treatment strategies (“Dora Richter,”2019). In 1979 The World Professional Association for Transgender Health (WPATH) was founded and published their first version of the Standards of Care (SOC) for the Health of Transsexual, Transgender, and Gender Nonconforming People (“WPATH,” 2019). Currently, WPATH is on their seventh version of the SOC which is opening doors for the treatment of this population.
With the rise of individuals who identify as transgender, gender non-binary and intersex, healthcare professionals have equally seen an influx of patients who require care throughout their discovery and transition. Though medical intervention for these individuals is not new, the first documented surgery was in 1922 to Dora Richter, it has often been segmented and lacking in evidence-based treatment strategies (“Dora Richter,”2019). In 1979 The World Professional Association for Transgender Health (WPATH) was founded and published their first version of the Standards of Care (SOC) for the Health of Transsexual, Transgender, and Gender Nonconforming People (“WPATH,” 2019). Currently, WPATH is on their seventh version of the SOC which is opening doors for the treatment of this population.
Though organizations such as WPATH have attempted to standardized care, the patient experience and reception of quality care are significantly lacking. In 2015 the National Center for Transgender Equality performed a groundbreaking survey of 27,215 respondents with the aim to “understand the lives and experiences of transgender people in the United States and the disparities that many transgender people face” (“About,”n.d., para. 1). This survey revealed that 33% of individuals who saw a health care provider had at least one negative experience related to being transgender (National Center for Transgender Equality, 2015). Negative experiences included; being refused treatment, verbal harassment, physically or sexually assault, and teaching the provider about transgender people in order to get appropriate care (National Center for Transgender Equality, 2015). Alternatively, 23% of respondents did not see a doctor when they needed to because of fear of being mistreated as a transgender person (National Center for Transgender Equality, 2015). Though these statistics are staggering and affronting there is hope for a better future.
Research for the care of these patients, specifically related to pelvic floor physical therapy, is on the rise. In the Annals of Plastic Surgery, an article was published with the purpose to capture incidence and severity of pelvic floor dysfunction pre-surgery, monitor any progression of symptoms with standardized outcome measures and highlight the role of physical therapy in the treatment of patients undergoing vaginoplasty (Manrique, et al., 2019). While in the Journal of Obstetrics & Gynecology a retrospective case series similarly focused on physical therapy pre and post-operatively highlighting dilator selection and success, pelvic floor dysfunction including bowel and bladder as well as reported abuse history (Jiang, Gallagher, Burchill, Berli, & Dugi, 2019). Through articles such as these clinicians can expect an uptick in calls questioning if they treat these patients. This begs the question of, "How can you best prepare?"
The answer is simple, attend continuing education. It is where you can not only learn evidence-based evaluation and treatment but also connect with other providers and mentors that care for these patients. In 2020 Herman & Wallace will be offering a continuing education course that serves this exact purpose. Keep your eyes on next years offerings, as spaces will surely fill quickly.
About. (n.d.). Retrieved May 15, 2019, from http://www.ustranssurvey.org/about
Dora Richter. (2019, May 09). Retrieved May 15, 2019, from https://en.wikipedia.org/wiki/Dora_Richter
Jiang, D. D., Gallagher, S., Burchill, L., Berli, J., & Dugi, D. (2019). Implementation of a Pelvic Floor Physical Therapy Program for Transgender Women Undergoing Gender-Affirming Vaginoplasty. Obstetrics & Gynecology,133(5), 1003-1011. doi:10.1097/aog.0000000000003236
Manrique, O. J., Adabi, K., Huang, T. C., Jorge-Martinez, J., Meihofer, L. E., Brassard, P., & Galan, R. (2019). Assessment of Pelvic Floor Anatomy for Male-to-Female Vaginoplasty and the Role of Physical Therapy on Functional and Patient-Reported Outcomes. Annals of Plastic Surgery,82(6), 661-666. doi:10.1097/sap.0000000000001680
National Center for Transgender Equality. (2015). Annual report of the U.S. Transgender Survey. Retrieved May 15, 2019, from https://transequality.org/sites/default/files/docs/usts/USTS-Executive-Summary-Dec17.pdf
Wpath. (n.d.). Standards of Care version 7. Retrieved May 15, 2019, from https://www.wpath.org/publications/soc

This post was written by the teaching team of Nancy Cullinane, PT, MSH, Kathy Golic, PT, and Terri Lannigan DPT, who took their talents to Nairobi, Kenya to teach a modified version of Herman & Wallace's Pelvic Floor Level 1 course.
 At the end of week 1 of Kenyan Pelvic Floor Level 1, we are pleased to report that 35 physiotherapists are embracing pelvic health physical therapy. Our students are primarily from the Nairobi area, however a handful have traveled from rural areas. The majority of them have some aspect of women's health in their job duties, however, only two have previously performed internal pelvic floor muscle techniques. On the first day of class, we spent significant introductory time discussing course objectives, students' clinical experience, Kenyan healthcare delivery, and what they hoped to gain from us. One student described teaching herself skills she is using in her clinical practice from watching YouTube videos. Another student commented, "the only tool I have to treat my patients is the kegel exercise and it isn't working for many of my patients. I know I'm missing something and I hope to find it here." The concept of internal pelvic floor muscle evaluation and treatment is new in Kenya and this is the first presentation of this coursework. There was significant anxiety surrounding internal pelvic muscle examination lab in the course. Several participants were not aware what "internal examination" meant in the course description when they registered. One student did not return on day two because of it. Nonetheless, as soon as the first internal assessment lab was completed, the pace picked up considerably.
At the end of week 1 of Kenyan Pelvic Floor Level 1, we are pleased to report that 35 physiotherapists are embracing pelvic health physical therapy. Our students are primarily from the Nairobi area, however a handful have traveled from rural areas. The majority of them have some aspect of women's health in their job duties, however, only two have previously performed internal pelvic floor muscle techniques. On the first day of class, we spent significant introductory time discussing course objectives, students' clinical experience, Kenyan healthcare delivery, and what they hoped to gain from us. One student described teaching herself skills she is using in her clinical practice from watching YouTube videos. Another student commented, "the only tool I have to treat my patients is the kegel exercise and it isn't working for many of my patients. I know I'm missing something and I hope to find it here." The concept of internal pelvic floor muscle evaluation and treatment is new in Kenya and this is the first presentation of this coursework. There was significant anxiety surrounding internal pelvic muscle examination lab in the course. Several participants were not aware what "internal examination" meant in the course description when they registered. One student did not return on day two because of it. Nonetheless, as soon as the first internal assessment lab was completed, the pace picked up considerably.
 These pioneering physiotherapists have developed new skills this past week for treating overactive bladder, mixed urinary incontinence, overactive pelvic floor muscles, prolapse, and diastasis recti. We have delved into discussion regarding sexual trauma and how cultural differences here in Kenya will impact the students' potential strategies in initiating conversations with their patients. Nine of our students are employed at Kenyatta National Hospital, the largest public hospital in Nairobi. Several are employed in private hospitals, who serve those citizens who pay to receive care in their respective systems. Many of our students are under-employed and some see patients privately in their homes, often for cash.
These pioneering physiotherapists have developed new skills this past week for treating overactive bladder, mixed urinary incontinence, overactive pelvic floor muscles, prolapse, and diastasis recti. We have delved into discussion regarding sexual trauma and how cultural differences here in Kenya will impact the students' potential strategies in initiating conversations with their patients. Nine of our students are employed at Kenyatta National Hospital, the largest public hospital in Nairobi. Several are employed in private hospitals, who serve those citizens who pay to receive care in their respective systems. Many of our students are under-employed and some see patients privately in their homes, often for cash.
We have additional Herman & Wallace Pelvic Floor Level 1 curriculum planned for week two, but we will also present the additional curriculum we have written specifically for these Kenyan physiotherapists. We will dedicate ample time toward connecting these motivated students with global mentoring resources, but we will also lay groundwork in helping them to set up a support network for pelvic health PT with each other.
We are honored and grateful to Herman & Wallace for donating Pelvic Floor Level 1 curriculum and to The Jackson Clinics Foundation for its history in changing physical therapy delivery in Kenya, including the financing of travel for this course. We are also thankful to Kenya Medical Training College for covering the cost of instructor lodging. At the half way mark of level 1, we feel we have already received so much more than we have given. We are especially grateful to the 35 course participants who will be changing the face of women's health physical therapy in Kenya from here on. Improving the quality of life for women improves the quality of life for families, and has an overall positive impact on the community.
The photography from this course is the creation of Marielle Selig, who acted as both technical support and official photographer for the Kenya Pelvic Floor Level 1 course. More of her work will be posted at https://mariselig.pixieset.com/.
All Upcoming Continuing Education Courses

Rehabilitative Ultrasound Imaging Pelvic Health Satellite Lab Course - Self-Hosted - April 17 - 19 2026
Apr 17 2026 - Apr 19 2026

Rehabilitative Ultrasound Imaging Pelvic Health Satellite Lab Course - Edmond OK - April 17 - 19 2026
Apr 17 2026 - Apr 19 2026

Pelvic Function Level 2B - Satellite - Bethpage NY - April 18 - 19 2026 - SOLD OUT
Apr 18 2026 - Apr 19 2026

Pelvic Function Level 1 - Satellite - Seattle WA - April 18 - 19 2026 - SOLD OUT
Apr 18 2026 - Apr 19 2026

Pelvic Function Level 1 - Satellite - Salt Lake City UT - April 18 - 19 2026 - SOLD OUT
Apr 18 2026 - Apr 19 2026

Pelvic Function Level 1 - Satellite - Newberg OR - April 18 - 19 2026 - SOLD OUT
Apr 18 2026 - Apr 19 2026

Menopause Transitions and Pelvic Rehab - Remote Course - April 18 - 19 2026
Apr 18 2026 - Apr 19 2026

Pelvic Function Level 1 - Satellite - Wichita KS - April 18 - 19 2026 - SOLD OUT
Apr 18 2026 - Apr 19 2026

Oncology of the Pelvic Floor Level 2A - Remote Course - April 18 - 19 2026
Apr 18 2026 - Apr 19 2026



Pelvic Function Level 1 - Satellite - St. Augustine FL - April 18 - 19 2026
Apr 18 2026 - Apr 19 2026

Pelvic Function Level 1 - Satellite - Minneapolis MN - April 18 - 19 2026 - SOLD OUT
Apr 18 2026 - Apr 19 2026



Pelvic Function Level 1 - Satellite - Colorado Springs CO - April 18 - 19 2026
Apr 18 2026 - Apr 19 2026













Pelvic Function Level 2B - Satellite - Nashotah WI - May 9 - 10 2026 - SOLD OUT
May 9 2026 - May 10 2026


Mobilization of the Myofascial Layer - Satellite Lab Course - Torrance CA - May 15 - 17 2026
May 15 2026 - May 17 2026
Mobilization of the Myofascial Layer - Satellite Lab Course Self-Hosted - May 15 - 17 2026
May 15 2026 - May 17 2026

Mobilization of the Myofascial Layer - Satellite Lab Course - McKinney TX - May 15 - 17 2026
May 15 2026 - May 17 2026

Mobilization of the Myofascial Layer - Satellite Lab Course - Bradenton FL - May 15 - 17 2026
May 15 2026 - May 17 2026

Mobilization of the Myofascial Layer - Satellite Lab Course - Atlanta GA - May 15 - 17 2026
May 15 2026 - May 17 2026

Pediatrics Level 2 - Adv Pediatric Bowel and Bladder Disorders - Remote Course - May 16 - 17 2026
May 16 2026 - May 17 2026


Pelvic Function Level 1 - In-Person - Bridgewater NJ - May 16 - 17 2026 - SOLD OUT
May 16 2026 - May 17 2026


