

At Herman & Wallace, we’re committed to making your educational experience as seamless, enriching, and applicable as possible—whether you're attending your first course or your fifteenth. As part of that mission, we offer several course formats and provide comprehensive pre-course resources through Teachable, our learning management system.
We recognize that every learner and every schedule is different. So, whether you're joining us from your home office or stepping into a clinic for a hands-on lab, here's a breakdown of what to expect.
1. Remote Courses (Live-Online)
These courses are delivered in real time over Zoom, allowing you to engage with faculty, ask questions, and participate in group discussions from anywhere with internet access. Ideal for those looking to minimize travel while still enjoying live interaction.
Includes:
- Pre-recorded lectures via Teachable (to be completed before the live Zoom session)
- Live labs, case studies, and group interaction via Zoom
- Real-time Q&A with instructors
2. Satellite-Lab Courses
Satellite courses blend the convenience of a local setting with the rigor of supervised lab instruction. Participants gather in small groups at designated satellite locations where a vetted teaching assistant facilitates the lab experience.
Includes:
- Live Zoom lectures from an off-site instructor, viewed together on-site
- Hands-on lab work completed in pairs or trios under the guidance of a teaching assistant
- Collaborative, small-group setting without requiring instructor travel
This model allows participants to get expert-led instruction and supervised lab training without needing to travel to a central location, making it a great middle-ground format.
3. In-Person Courses
For those who thrive in hands-on, face-to-face environments, our in-person courses are held at host clinics across the country. These offer an immersive learning experience with practical labs and direct faculty mentorship during the course.
Includes:
- Pre-course content on Teachable (depending on the course)
- On-site training with small group lab instruction
- Networking opportunities with peers and instructors
4. Self-Hosted Courses
For experienced therapists looking for maximum flexibility, Self-Hosted Courses allow small groups of licensed participants to learn together independently. This format is available for select intermediate and advanced courses and requires prior completion of foundational lab work with instructor supervision.
Includes:
- Live lectures via Zoom, viewed by your self-organized group at a location of your choosing
- Lab work completed without a teaching assistant, but in compliance with all safety and ethical standards
- Access to Teachable for pre-course content, handouts, and required equipment lists
Important Requirements:
- All participants must be licensed therapists and registered for the course
- Lab partners must be fellow licensed participants—no patients or unlicensed individuals
- Ideal for clinic teams or colleagues with a strong foundation in pelvic rehab
Teachable Pre-Course Access: Set Yourself Up for Success
Once you register for a Herman & Wallace course, you’ll receive access to the Teachable platform, where you'll find essential materials to review before the live or in-person session.
Here’s what’s typically included:
- Course Agenda & Zoom Links: You’ll find a detailed course schedule, so you know exactly what to expect, as well as Zoom links for remote sessions.
- Pre-Recorded Lectures: Many courses offer pre-recorded didactic material that must be completed before the live component. This helps maximize hands-on time during your live sessions.
- Supplemental Readings & Handouts: Downloadable PDFs, journal articles, and anatomical diagrams may be included to reinforce key concepts.
- Required Equipment Lists: For remote lab-based courses, you’ll see a list of items you'll need for lab participation—like towels, pillows, or therapy tools—so you're fully prepared.
- Post-Course Content: All courses include and require you to complete a post-course test and evaluation to receive the course certificate.
⏳ When Should You Start Reviewing Teachable Content?
We recommend logging into Teachable and reviewing the course materials at least 2-3 weeks prior to the course date. Some content is required for course participation, especially for remote courses, and you may need time to gather supplies or complete prerequisite videos.
💡 Pro Tips for a Smooth Experience
Bookmark Teachable: Make sure you’re signed up with the correct email and can easily log in.
Download Materials in Advance: Don’t wait until the day of the course—PDFs and lecture slides are often available early.
Check the Agenda Carefully: Some courses span multiple days or include breaks—plan your time accordingly.
Your Education, Elevated
Whether you're just entering the field of pelvic rehabilitation or deepening a specialized area of practice, Herman & Wallace’s diverse course formats are designed to support your learning style, schedule, and clinical needs. With Teachable providing centralized access to all your course content, you're never starting from scratch.
Explore upcoming courses at www,hermanwallace.com/continuing-education-courses and take the next step in your pelvic health education journey.


At Herman & Wallace, we know that pelvic rehabilitation is a dynamic and ever-evolving field. While foundational courses like Pelvic Function Level 1 and Dry Needling and Pelvic Health often get the spotlight, there are several highly valuable courses that tend to fly under the radar. These courses offer practitioners the opportunity to deepen their knowledge, broaden their skills, and better serve patients with complex needs.
Here are five underrated courses that can have a powerful impact on your practice:
1. Nutrition Perspectives for the Pelvic Rehab Therapist
 Pelvic health doesn’t exist in isolation from the rest of the body, and nutrition plays a critical role in tissue healing, inflammation, digestion, and pelvic pain syndromes. This course introduces pelvic rehab practitioners to the fundamentals of nutrition as it relates to pelvic health.
Pelvic health doesn’t exist in isolation from the rest of the body, and nutrition plays a critical role in tissue healing, inflammation, digestion, and pelvic pain syndromes. This course introduces pelvic rehab practitioners to the fundamentals of nutrition as it relates to pelvic health.
Participants learn how to recognize when dietary factors may be contributing to issues such as constipation, bladder irritation, vulvar pain, or chronic inflammation. While not a course that trains clinicians to act as dietitians, it empowers them to screen for red flags, collaborate with nutrition professionals, and make basic, evidence-informed recommendations that can significantly impact patient outcomes.
2025 Course Date Options: October 11-12, December 6-7.
2. Oncology and the Pelvic Floor Series
 (OPF1: Foundations, OPF2A: Male Pelvic & Colorectal Cancers, and OPF2B: Female Pelvic & Bladder Cancers)
(OPF1: Foundations, OPF2A: Male Pelvic & Colorectal Cancers, and OPF2B: Female Pelvic & Bladder Cancers)
Pelvic health isn’t just for perinatal or orthopedic populations. People undergoing treatment for pelvic and abdominal cancers face unique and complex challenges, including incontinence, pelvic pain, sexual dysfunction, and scar tissue restrictions.
The Oncology and the Pelvic Floor series offers a comprehensive framework for working with patients at every stage of the cancer journey, and provides the knowledge and sensitivity needed to support this underserved population, integrating trauma-informed care, manual therapy, exercise, and interdisciplinary collaboration.
2025 Course Date Options: Level 1 September 13-14, Level 2A December 6-7, Level 2B November 1-2.
3. Pharmacologic Considerations for the Pelvic Health Provider
 Medications have a profound impact on the pelvic floor—often in ways that are overlooked. Whether it’s constipation from opioids, hormonal changes from contraceptives, or bladder irritation from certain antibiotics, understanding pharmacology is crucial.
Medications have a profound impact on the pelvic floor—often in ways that are overlooked. Whether it’s constipation from opioids, hormonal changes from contraceptives, or bladder irritation from certain antibiotics, understanding pharmacology is crucial.
This course demystifies medications commonly encountered in pelvic health practice. It helps clinicians understand how drugs can influence bowel, bladder, sexual function, pain processing, and healing. Armed with this knowledge, practitioners can engage in more informed discussions with patients and other members of the healthcare team, helping to troubleshoot barriers to progress.
2025 Course Date Option: September 13.
4. Yoga for Pelvic Pain
 Yoga is more than stretching—it’s a mind-body practice with proven benefits for nervous system regulation, pain management, and muscular balance. Yoga for Pelvic Pain teaches practitioners how to integrate evidence-based yoga principles into rehabilitation for patients with chronic pelvic pain.
Yoga is more than stretching—it’s a mind-body practice with proven benefits for nervous system regulation, pain management, and muscular balance. Yoga for Pelvic Pain teaches practitioners how to integrate evidence-based yoga principles into rehabilitation for patients with chronic pelvic pain.
This course goes beyond asana (physical postures) to incorporate breathwork, mindfulness, and gentle movement tailored to the needs of people with complex pain syndromes. Participants leave with practical tools they can immediately incorporate into one-on-one sessions or group classes, supporting both physical function and emotional well-being.
2025 Course Date Option: September 13-14.
5. Rehabilitative Ultrasound Imaging: Pelvic Health & Orthopedic Topics
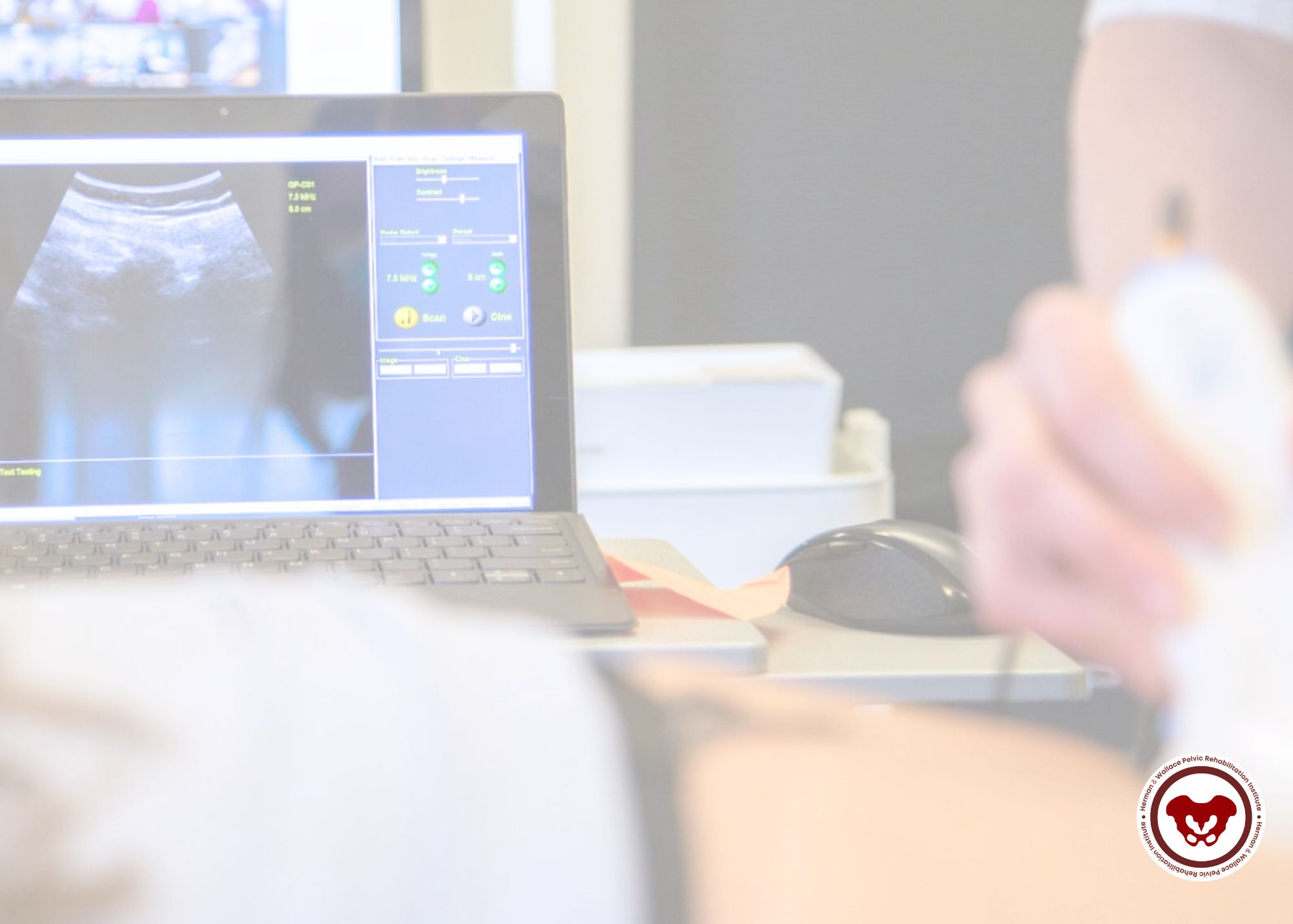 Rehabilitative Ultrasound Imaging (RUSI) provides real-time feedback for both clinicians and patients. It’s an invaluable tool for assessing muscle activation, motor control, and coordination - particularly for the deep core and pelvic floor muscles.
Rehabilitative Ultrasound Imaging (RUSI) provides real-time feedback for both clinicians and patients. It’s an invaluable tool for assessing muscle activation, motor control, and coordination - particularly for the deep core and pelvic floor muscles.
This course covers both pelvic health applications (like visualizing pelvic floor contractions) and broader orthopedic topics (like assessing the transverse abdominis or multifidus). Practitioners gain hands-on experience in using ultrasound to refine exercise prescription, improve patient engagement, and objectively document progress. Despite its transformative potential, RUSI remains underutilized in many pelvic rehab settings.
2025 Course Date Options for September 5-7: Self-hosted, Indianapolis IN, Seattle WA.
Don’t Overlook These Gems
Expanding your clinical toolbox with specialized knowledge can transform your patient care. Whether it’s understanding how nutrition, medications, cancer treatments, or mind-body practices influence the pelvic floor—or learning to harness the power of ultrasound imaging—these courses provide essential insights that go beyond the basics.
Ready to elevate your practice? Explore these courses and others at Herman & Wallace and continue your journey as a lifelong learner in pelvic rehabilitation.

Working with children in pelvic rehabilitation is a deeply meaningful and highly specialized area of practice. It also comes with unique ethical responsibilities. Pediatric pelvic health involves treating conditions such as enuresis, constipation, pelvic floor dysfunction, and developmental delays — all within the context of a child’s developing autonomy, family dynamics, and sensitive anatomical areas.
As clinicians, our ethical frameworks must evolve to accommodate not only clinical best practices but also the emotional, developmental, and psychosocial needs of the child.
Here, we examine the critical ethical principles that should guide our work in pediatric pelvic rehab.
Consent, Assent, and Autonomy
Unlike adult patients, children cannot legally provide informed consent — this must be obtained from a parent or legal guardian. However, ethical practice also requires assent from the child: their affirmative agreement to participate in the therapy process. This includes:
- Explaining the treatment plan in age-appropriate language
- Respecting a child's refusal or hesitation
- Avoiding coercion, even indirectly, from caregivers
When working in the pelvic region, where the potential for discomfort or boundary violation is high, ongoing, iterative assent is essential. Even young children have a right to bodily autonomy and should feel empowered to say “no” at any time.
Scope of Practice and Referral Boundaries
Pediatric pelvic dysfunction can sometimes signal deeper issues: developmental disorders, psychosocial stressors, or even trauma. Therapists must maintain clarity around scope of practice, referring out when behavioral or psychological concerns arise that are beyond the purview of physical therapy.
Examples include:
- Suspected abuse or trauma history
- Complex toileting behaviors tied to anxiety, OCD, or family systems
- Significant delays in emotional regulation or sensory integration
Collaborative care — with pediatricians, psychologists, occupational therapists, and social workers — is often essential for truly holistic treatment.
Privacy and the Triadic Relationship (Child–Parent–Therapist)
Pediatric pelvic rehab takes place in a triadic dynamic: therapist, child, and caregiver. This requires delicate communication boundaries. While transparency with caregivers is important, so is the child’s right to privacy, particularly as they age into adolescence.
Key ethical questions to consider:
- How much of the session content should be shared with parents?
- Does the child want to speak with the therapist alone?
- Are we creating a space where the child can speak freely without fear of being reported back to their parent?
Navigating this triad ethically means validating the caregiver's role while protecting the developing autonomy and emotional safety of the child.
Touch and Trauma Sensitivity
Because pelvic therapy inherently involves close proximity to intimate body regions, we must always practice trauma-informed care, regardless of the child’s known history. That includes:
- Using neutral, non-threatening language to describe anatomy
- Modeling consent with every interaction
- Offering alternatives to internal assessment (e.g., external palpation, biofeedback, or movement-based therapy)
- Ensuring the child never feels “examined,” but instead “participates” in treatment
Even well-intentioned treatment can be experienced as invasive if delivered without attunement to the child’s comfort and nervous system cues.
Gender Diversity and Inclusive Care
As gender-diverse children and adolescents become more visible in healthcare, it is ethically incumbent upon us to provide affirming, inclusive care. This includes:
- Using the child’s chosen name and pronouns
- Avoiding assumptions about anatomy, gender identity, or toileting goals
- Providing education and support for caregivers navigating unfamiliar terrain
If you’re not yet comfortable or informed in this area, seek training — not just for ethical compliance, but to provide competent and compassionate care.
Documentation and Legal Reporting
Ethical practice in pediatric care also includes accurate, sensitive documentation — especially when required to interface with schools, insurance providers, or legal systems.
Additionally, as mandated reporters, pelvic health professionals must know the signs of possible abuse or neglect and report concerns appropriately. This responsibility is both legal and ethical and should never be avoided due to discomfort or fear of disrupting rapport.
Ethical care in pediatric pelvic health is not just about following rules — it’s about respecting the whole child, honoring their voice, and creating a space where healing can happen safely. In this sensitive area of practice, our ethics must be as carefully honed as our clinical skills.
Through trauma-informed care, developmental awareness, and collaborative practice, we can offer children and families the support they need — while upholding the highest ethical standards of our profession.
Take the next step in this learning journey, and earn your ethics CEUS by joining Mora Pluchino, PT, DPT, PRPC, in Ethical Considerations for Pediatric Pelvic Health on July 27th. This one-day remote course covers ethical considerations for professionals working in the area of pediatric pelvic health. In general, healthcare professionals have many day-to-day ethical considerations to “do no harm.” This includes fundamental decisions related to billing, patient care, safety, and compliance.

There’s something special about gathering in a room with colleagues, exchanging ideas, practicing hands-on techniques, and learning from expert instructors in real time. While virtual education offers flexibility and accessibility, many pelvic health practitioners are eager to get back to the connection, feedback, and tactile learning that only in-person courses can provide.
If you’re ready to step back into a live classroom, Herman & Wallace has a robust lineup of in-person courses designed to sharpen your clinical skills, deepen your understanding of pelvic health, and connect you with a like-minded community of learners.
Here are some of the in-person courses currently offered:
Pelvic Function Series (In Person)
This progressive pathway is ideal for clinicians looking to build their foundation and then layer on advanced skills.
- Pelvic Function Level 1 – A great entry point into pelvic rehabilitation, this foundational course provides a whole-body framework to assess and treat pelvic floor dysfunction. You’ll gain essential hands-on skills and clinical reasoning strategies.
-
-
- Boston MA - September 6-7
- Detroit MI - November 15-16
- New York NY - December 21-22
-
- Pelvic Function Level 2A, 2B, and 2C – These courses dive deeper into the muscular, fascial, and neurological systems affecting pelvic function. Each level builds upon the previous one, covering complex diagnoses and interventions with plenty of lab time for integration.
-
- Level 2A – Expand your skills in colorectal pelvic health, pudendal neuralgia, and coccyx pain
- Richmond VA - August 9-10
- St. Paul MN - September 13-14
- New York NY - May 31 - June 1
- Level 2B – Expand your skills in pelvic pain, urogynecologic examinations, and treatment options
- Houston TX - June 28-29
- Atlanta GA - September 6-7
- Baltimore MD - September 20-21
- Houston TX - October 4-5
- Richmond VA - November 15-16
- Level 2C – Expand your skills in men’s pelvic health and rehabilitation
- Colorado Springs CO - October 4-5
- Level 2A – Expand your skills in colorectal pelvic health, pudendal neuralgia, and coccyx pain
- Modalities and Pelvic Function – Want to add tools like biofeedback, electrical stimulation, or dry needling to your practice? This course teaches the safe and effective use of modalities within the context of pelvic rehab and pelvic pain.
-
-
- Houston TX - July 12-13
- Akron OH - September 20-21
- Somerset NJ - October 4-5
-
Specialty In-Person Courses
Dry Needling and Pelvic Health Series (In Person) – This hands-on series provides targeted training in the use of dry needling for pelvic conditions.
- Dry Needling and Pelvic Health: Pregnancy – This specialty course explores the safe application of dry needling during pregnancy. Learn how to integrate this modality into perinatal care with a strong emphasis on patient safety, comfort, and outcomes.
-
- Lemont IL - August 23-2
- Dry Needling and Pelvic Health Level 2 – Designed for clinicians who have completed the foundational dry needling course, this course focuses on advanced techniques for addressing pelvic floor and associated neuromusculoskeletal dysfunctions.
Dunluth MN - August 2-3
Pessaries and Pelvic Rehab – Gain hands-on training in assessing, fitting, and managing pessaries for pelvic organ prolapse and incontinence. Learn clinical considerations and practice fitting techniques in supervised labs.
- Chicago IL - November 8-9
- Tacoma WA - January 31 - February 1
High Intensity Perinatal Athletics Practicum –Designed for practitioners working with pregnant and postpartum athletes, this course blends lecture and lab to address clinical decision-making in high-intensity training contexts like CrossFit, HIIT, and Olympic lifting. Understand how to keep your athletic patients safe and strong throughout the perinatal period.
- Somerset NJ - September 27-28
Ready to Join Us In Person?
Whether you’re just starting out or expanding your advanced skills, Herman & Wallace offers a wide range of in-person courses to support your clinical growth. Don’t miss this opportunity to step away from your screen and back into the dynamic environment of hands-on learning.
Explore the full calendar of in-person courses and reserve your spot today. Spaces are limited and tend to fill quickly!

Pelvic rehabilitation professionals know that working with athletes requires a unique lens—and when your client is both an athlete and navigating the perinatal period, the clinical complexity deepens.
That’s why Herman & Wallace is excited to announce the High Intensity Perinatal Athletics Practicum, coming to Somerset, NJ on September 27–28, 2025. This two-day course is built for pelvic rehab practitioners who want to elevate their skills in evaluating and treating pregnant and postpartum individuals engaging in high-intensity interval training (HIIT), including activities like weightlifting, gymnastics, plyometrics, and running.
The practicum blends pre-course videos, targeted in-person lectures, and hands-on movement labs. You'll explore:
- Biomechanics and breathing strategies tailored for the perinatal athlete
- Technique review and movement modifications to support performance and healing
- Practical tools for managing pelvic symptoms in high-level exercisers
- Manual therapy techniques specific to this population
Participants should come prepared to move—exercise attire is encouraged for active lab sessions that put knowledge into motion.
Whether you're treating CrossFit athletes, recreational runners, or competitive lifters, this course will give you the confidence to work safely and effectively with perinatal clients committed to staying active.
Prerequisite: Completion of Pelvic Function Level 1 through Herman & Wallace or Pelvic PT 1 through the APTA.
Ready to take your clinical practice to the next level?
Secure your spot in the High Intensity Perinatal Athletics Practicum in Somerset, NJ the weekend of September 27-28th, and empower your work with evidence-based strategies for supporting athleticism in the perinatal journey.

Gender-affirming vaginoplasty is a major surgical milestone in the gender transition process for many transfeminine individuals. As pelvic rehabilitation therapists, we play a critical role in supporting these patients post-operatively — particularly with respect to wound healing, dilation adherence, pelvic floor muscle function, and the resumption or initiation of sexual activity. An informed, trauma-aware, and affirming approach is essential to help optimize long-term outcomes and quality of life for transgender and nonbinary (TGNB) individuals.
Understanding Vaginoplasty and the Role of Dilation
Vaginoplasty creates a vaginal canal. Successful outcomes depend on surgical technique, tissue health, post-operative care, and patient adherence to dilation protocols. Dilation is essential for maintaining the patency and depth of the neovaginal canal, especially in the first year post-surgery when wound healing and scar tissue remodeling are most active. It is critical for patients to understand that the purpose of dilation is not just to preserve depth but also to promote scar mobility, reduce adhesions, and support sensory adaptation.
Dilation protocols vary slightly depending on the surgeon and the patient’s healing course. General phases include:
- Early post-op (Weeks 1–6): Patients are usually instructed to dilate 3-4 times per day. This phase aligns with active wound healing and high tissue reactivity.
- Subacute phase (Weeks 6–12): Frequency gradually decreases to 2–3 times per day as epithelialization occurs and inflammation subsides.
- Maintenance phase (3–12 months and beyond): Most patients are advised to continue dilation at least once daily or several times per week, depending on sexual activity levels and individual tissue response.
Sexual activity that involves vaginal penetration may substitute for some dilation sessions, but not entirely, especially early in the healing process. Patients must understand the purpose of dilation as not just preserving depth, but also promoting scar mobility, reducing adhesions, and supporting sensory adaptation.
Several factors can lead to adaptations in standard dilation protocols:
- Tissue source: When penile inversion alone is insufficient (e.g., due to lack of available skin), surgeons may use peritoneal grafts. This will mean two circumferential incisions. Some surgeons recommend dilation on day 6 post-op.
- Healing complications: Hypergranulation, infection, or partial dehiscence may lead to modifications in dilation. In such cases, rehab professionals must coordinate with the surgical team.
- Patient pain or dysphoria: Dilation can be a source of emotional and physical discomfort. This can lead to avoidance behaviors, increasing the risk of canal stenosis. Trauma-informed approaches and graded exposure are key strategies for rehab professionals to support patients in maintaining consistent dilation.
Sexual function following vaginoplasty is deeply personal and multifactorial. While surgical outcomes focus on aesthetics and depth, sensory outcomes can vary, depending largely on nerve preservation (especially the dorsal nerve of the penis) and individual healing. Sexual activity that involves vaginal or anal penetration is contraindicated in the first 12 weeks of the healing process.
Pelvic rehabilitation therapists may encounter:
- Pelvic floor hypertonicity or guarding: Fear, trauma history, or dilation discomfort can result in involuntary protective muscle patterns, contributing to pain with penetration or dilation.
- Lack of sensory feedback: Some patients report numbness or muted sensation in the neovagina, which can influence arousal and engagement in sexual activity.
- Functional impairments: Scar adhesions, stenosis, or asymmetry may affect function. Self-care with graded dilation, varying the type of dilator used, using the dilator to stretch the puborectalis, or using wearable dilators at night may be beneficial.
Affirming sexual health education — including discussion of lubrication products, positioning, and sensate mapping — is within the scope of a knowledgeable pelvic rehab provider. Supporting patients in developing trust in their bodies, understanding their anatomy, and embracing pleasure is a valuable contribution to the post-vaginoplasty journey.
Working with people from the transgender-gender diverse community requires more than clinical expertise — it demands an ongoing commitment to inclusive, affirming care. Rehab professionals should:
- Use accurate, affirmed names and pronouns.
- Avoid assumptions about anatomy, orientation, or sexual goals.
- Create a safe environment for disclosure, exploration, and education.
As pelvic rehabilitation therapists, our expertise in supporting transgender patients through post-operative recovery is paramount. By understanding the intricate details of healing and functional outcomes associated with genital gender-affirming surgeries — such as vaginoplasty, phalloplasty, and metoidioplasty — we can better address patient concerns around urinary, bowel, pain, and sexual function. Our work also benefits from a comprehensive appreciation of the societal and medical experiences that shape the journeys of transgender individuals, as well as the health effects of hormones relevant to differential diagnosis in rehabilitation.
Ready to advance your skills and provide truly affirming care? Register for Transgender Health for the Rehab Professional on August 2, 2025, and join us for an in-depth exploration of genital gender-affirming surgeries, postoperative healing, and the broader context of transgender health care. Secure your spot today to elevate your practice and support your patients with the latest evidence-based strategies.
Resources
- Unger, C. A. (2016). Care of the transgender patient: Surgical and non-surgical options. Clinical Obstetrics and Gynecology, 59(1), 114–126. doi:10.1097/GRF.0000000000000160
- Schechter, L. S., et al. (2020). Primary vaginoplasty: Techniques and outcomes. Clinics in Plastic Surgery, 45(3), 361–370.
- Kaefer, M., et al. (2023). Transfeminine vaginoplasty: Postoperative complications and management. Urology Clinics of North America, 50(1), 125–138.
- Reisner, S. L., et al. (2015). Global health burden and needs of transgender populations: A review. The Lancet, 388(10042), 412–436. doi:10.1016/S0140-6736(16)00684-X
AUTHOR BIO:
Sandra Gallagher, PT, DPT, WCS
 Sandra Gallagher, PT, DPT, WCS (she/her) is a pelvic health physical therapist in Portland, OR. Her practice includes providing evaluation and treatment of pelvic health conditions in adults and children of all gender identities. Dr. Gallagher received her primary physical therapy training in 1986 with a BS in Physical Therapy from the University of Lowell in Massachusetts. She has pursued varied continuing education in manual therapy, Feldenkrais, biophysical agents, pelvic health, and pregnancy. She completed her Doctorate of Physical Therapy in June 2020.
Sandra Gallagher, PT, DPT, WCS (she/her) is a pelvic health physical therapist in Portland, OR. Her practice includes providing evaluation and treatment of pelvic health conditions in adults and children of all gender identities. Dr. Gallagher received her primary physical therapy training in 1986 with a BS in Physical Therapy from the University of Lowell in Massachusetts. She has pursued varied continuing education in manual therapy, Feldenkrais, biophysical agents, pelvic health, and pregnancy. She completed her Doctorate of Physical Therapy in June 2020.
Sandi has served on varied committees and boards at the state and national level, most recently as the chair of the CAPP-OBC committee for the Academy of Pelvic Health of the APTA. She has presented on the role of PT in gender affirming vaginoplasty at the UCSF Transgender Health Summit, APTA Combined Sections Meeting, and at the 2018 international meeting of the World Professional Association for Transgender Health (WPATH). She is the recipient of the 2020 Elizabeth Noble Award from the Academy of Pelvic Health.


Coccydynia, commonly referred to as tailbone pain, can be a profoundly limiting and misunderstood condition. Although it affects a relatively small percentage of patients, its impact on function and quality of life is often disproportionate to its size. As pelvic rehabilitation therapists, we are uniquely positioned to assess and treat the biomechanical, musculoskeletal, and neuromuscular contributors to coccydynia, especially when sitting becomes painful or intolerable.
Coccydynia is typically defined as pain in the coccyx region, often exacerbated by sitting, transitioning from sit to stand, or activities that increase pressure on the tailbone (e.g., biking or prolonged driving). While trauma, like a fall onto the tailbone or childbirth, is a common cause, many cases are idiopathic or associated with repetitive strain, postural dysfunction, or referred pain from nearby structures.
Some key contributors we see in clinical practice include coccygeal hypermobility or hypomobility, myofascial dysfunction (in pelvic floor muscles, gluteal, obturator internus, or levator ani muscles), lumbar/sacral or SI joint dysfunction, scarring or adhesions from previous surgeries or trauma, central sensitization, and chronic pain responses.
We can identify coccygeal mobility restrictions, myofascial tension, or biomechanical contributors by performing a thorough assessment and a combination of internal and external examinations. Key assessment components may include observation of seated posture and pelvic alignment. Palpation of coccyx and surrounding tissues externally and when appropriate, and consented to, internally. Evaluation of coccygeal mobility via rectal or vaginal exam. Screening for lumbar and sacroiliac joint dysfunction. Muscle tone assessment of pelvic floor and adjacent muscles, and Functional sitting tests and aggravating movements analysis.
Treatment Considerations
A multimodal treatment plan for coccydynia should be tailored to the root cause(s), and sensitive to the often-overlooked emotional burden of persistent sitting pain.
- Manual Therapy
- Internal coccyx mobilization: Often essential in addressing hypomobility or malalignment. Gentle ventral/dorsal glides can restore mobility.
- Myofascial release: Releasing obturator internus, coccygeus, piriformis, and other key muscles often alleviates referred pain.
- External techniques: Sacral mobilizations, soft tissue work to gluteal and lumbar areas.
- Postural and Ergonomic Re-education
- Patients may develop rigid, guarded postures to avoid pain. Education and cueing for neutral spine and dynamic sitting strategies are key.
- Use of coccyx cut-out cushions can immediately reduce pressure and allow for healing.
- Pelvic Floor Muscle Re-training
- Address overactivity or guarding in pelvic floor muscles.
- Down-training, biofeedback, and coordination exercises may be appropriate depending on the findings.
- Addressing Central Sensitization
- For chronic or severe cases, central nervous system sensitization may amplify symptoms.
- Incorporate pain neuroscience education, graded exposure, and nervous system regulation techniques (e.g., breathwork, mindfulness, or autonomic retraining).
Painful sitting is more than an inconvenience—it can become a barrier to work, relationships, travel, and participation in daily life. As pelvic rehab specialists, we have the skills to bring validation, relief, and long-term strategies to people with coccydynia. By blending hands-on techniques with nervous system support, posture retraining, and education, we can help patients reclaim comfort and confidence in their bodies—one seat at a time.
If you're ready to deepen your clinical reasoning and expand your toolbox for treating coccydynia, we invite you to join Lila Abbate, PT, DPT, OCS, WCS, PRPC, for the remote course Coccydynia and Painful Sitting on August 2, 2025. Lila brings decades of pelvic health experience and a dynamic, practical approach to treating coccyx-related pain. Don’t miss this opportunity to sharpen your assessment and intervention skills for one of the most under-treated yet impactful pelvic pain conditions.
Register now to secure your spot and transform how you approach coccyx pain in your practice.
References:
- Dufour, S., Vandyken, B., & Carter, M. (2018). Pelvic Girdle Pain and Dysfunction: A Clinical Guide. Handspring Publishing.
- Hesch, J. (2015). The Hesch Method of Treating Coccyx Dysfunction. International Journal of Osteopathic Medicine, 18(1), 50–57. https://doi.org/10.1016/j.ijosm.2014.09.003
- Bordoni, B., & Varacallo, M. (2024). Anatomy, Back, Coccygeal Muscles. In StatPearls. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK538485/


As pelvic rehabilitation therapists, we are uniquely positioned to deliver care that honors both the physical and emotional complexities of each patient's body. Our field often involves working intimately with anatomy, which means it's essential to provide affirming, informed, and inclusive care for all individuals, including those who are intersex.
The intersection of pelvic rehabilitation and intersex health demands not only biomechanical insight but also a sophisticated, embodied understanding of trauma, identity, and consent. As clinicians working within the intimate landscapes of the pelvis, we must widen our therapeutic lens to serve the needs of intersex individuals — those born with variations that fall outside binary definitions of male or female bodies.
Intersex variations (sometimes referred to as DSDs, or differences of sex development — though this term remains controversial) include a wide spectrum of chromosomal, gonadal, hormonal, and anatomical variations. These include, but are not limited to: Androgen Insensitivity Syndrome (AIS), Congenital Adrenal Hyperplasia (CAH), Klinefelter syndrome (XXY), Turner syndrome (XO), 5-Alpha-Reductase Deficiency, and mixed gonadal dysgenesis.
Medicalization, Trauma, and the Pelvic Therapist’s Role
Historically, intersex bodies have been subject to significant medical pathologization — often resulting in non-consensual “normalizing” surgeries in infancy or early childhood. These procedures, which aim to produce phenotypically male or female anatomy, are increasingly condemned by human rights organizations and intersex-led advocacy groups as unnecessary and harmful.
These non-consensual, non-medically necessary procedures can cause lifelong trauma, and can result in chronic pelvic pain, scar tissue, altered sensation, urinary or bowel dysfunction, and profound psychological trauma.
As pelvic therapists, we are uniquely positioned to address not only the myofascial and neurovascular sequelae of such surgeries but also to support patients in reclaiming agency, sensation, and choice in their own bodies. Clinical goals might include:
- Scar mobilization and desensitization
- Pelvic floor muscle coordination training
- Strategies for comfort with intercourse
- Voiding retraining or bowel programs
- Support for body awareness and reconnection with pelvic sensation
Clinical Considerations
- Anatomical Complexity and Variance
Be prepared to encounter nonstandard presentations of genital, pelvic, and abdominal anatomy. Surgical techniques may have altered the course of neurovascular bundles or led to neuromas, tethered scars, or dysesthetic tissue.
Advanced internal assessment should always be prefaced with explicit, iterative consent. In some cases, conventional intravaginal or intrarectal assessment is neither appropriate nor psychologically safe. Use external and visual inspection, gentle palpation, biofeedback, and motion-based functional assessment to build rapport and collect data noninvasively.
- Functional Sequelae
Common presenting concerns may include:
- Dyspareunia or difficulty with comfortable intercourse
- Poor coordination or overactivity of pelvic floor muscles post-vaginoplasty or hypospadias repair
- Scar restriction or neuromuscular disruption following gonadectomy or other abdominal procedures
- Voiding dysfunction, urethral hypersensitivity, or chronic perineal pain
- Dissociation or disconnection from pelvic sensation and identity
Customized, layered intervention may include myofascial mobilization, visceral manipulation, pelvic floor retraining, bowel/bladder retraining, and somatosensory reintegration techniques that emphasize curiosity, neutrality, and embodiment.
- Trauma Stewardship
Intersex patients may experience a compounded burden of trauma — developmental, medical, and social. Understand the neurophysiologic imprint of chronic invalidation, coercion, and boundary violation. Clinicians should cultivate a regulated therapeutic presence and understand signs of autonomic dysregulation (e.g., freeze response, fawning, shutdown) during assessment and manual interventions.
Avoid defaulting to protocols. Build safety through co-created treatment plans, anchored in shared language, flexible pacing, and ongoing attunement.
- Hormone Histories and Tissue Response
Some intersex patients have to take hormones due to their variation producing lower than typical amounts of hormones or due to non-consensual procedures, some intersex folx have to take hormones as supplements/replacements. Hormones can impact tissue elasticity, hydration, healing capacity, and pelvic vascularization.
Coordinate with endocrinology and gyne/urology to stay updated on hormone dosing, surgical outcomes, and relevant lab findings.
Inclusive Documentation and Systems Change
Advanced practice extends beyond the treatment room. Systems must reflect inclusive, patient-centered values. This includes:
- Non-binary anatomical charts and intake forms
- EHR templates that accommodate non-binary sex markers and customizable anatomy fields
- Consent forms that separate pelvic floor therapy from general physical therapy
- Language policies that prioritize lived experience over assigned sex or diagnosis codes
If your clinical environment does not support this yet, consider yourself the culture-change agent. Clinical excellence includes advocacy.
Reflective Practice and Positionality
As clinicians, our understanding of “normal” anatomy, function, and gender is shaped by our training and culture. Working with intersex patients requires ongoing reflection:
- Where did I learn what “female” and “male” anatomy looks like?
- How do I manage uncertainty or ambiguity in my assessments?
- Am I comfortable being the learner in the room?
Deeply inclusive care requires humility, curiosity, and cultural literacy. It asks us not just to treat, but to listen, witness, and validate the lived reality of bodies that have too often been pathologized.
Intersex patients are not rare; they are underserved. As pelvic rehab providers operating at the nexus of anatomy, trauma, and embodiment, we have a profound opportunity — and responsibility — to make our care spaces safer, more skillful, and more just. This is not a fringe issue. It is core to ethical, person-centered pelvic health care.
For pelvic health professionals seeking to deepen their knowledge and clinical competency, the Intersex Patients: Rehab and Inclusive Care course instructed by Molly O'Brien-Horn, PT, DPT, CLT provides an essential next step. This course expands on the clinical and ethical considerations discussed here, offering advanced instruction in trauma-informed care, inclusive communication, and hands-on strategies for working with diverse intersex anatomies. By engaging in this training, clinicians not only sharpen their therapeutic skills but also actively participate in a broader movement to dismantle medical harm and restore autonomy, dignity, and agency to intersex individuals in the healthcare system.
Intersex Patients: Rehab and Inclusive Care is scheduled for August 23 and November 8, 2025.
Resources:
- Lee PA, et al. “Consensus Statement on Management of Intersex Disorders.” Pediatrics. 2006;118(2):e488–500.
- Karkazis K. Fixing Sex: Intersex, Medical Authority, and Lived Experience. Duke University Press; 2008.
- Roen K. “Intersex Embodiment: Variations of Sex Development and the Politics of Touch.” Feminism & Psychology. 2019;29(2):157–74.
- Liao LM, et al. “Non-Consent and ‘Disorders of Sex Development.’” Bioethics. 2010;24(9):490–97.
- Creighton SM, Minto CL, Steele SJ. “Objective Cosmetic and Anatomical Outcomes at Adolescence of Feminising Surgery for Ambiguous Genitalia Done in Childhood.” The Lancet. 2001;358(9276):124–25.


As pelvic rehabilitation continues to evolve, so does our understanding of how to access and modulate the intricate neuromuscular systems that govern pelvic floor function.
Dry needling — long employed in orthopedic and sports medicine settings — is now emerging as a potent tool in the pelvic health therapist’s repertoire. Its precise application can yield neurophysiologic effects far beyond simple trigger point release, particularly when integrated with a broader neuromodulation framework.
The Rationale for Dry Needling in Pelvic Health
Dry needling involves the insertion of a monofilament needle into myofascial, peri-neural, or connective tissues to elicit a therapeutic response. In the pelvic region — where layered dysfunction may involve somatic, autonomic, and visceral pathways — dry needling offers:
- Direct modulation of overactive or inhibited pelvic floor muscles
- Reduction of peripheral nociceptive input from sensitized tissues
- Central downregulation of pain pathways through segmental and supraspinal mechanisms
- Neurovascular and neuroimmune effects that influence tissue health and pelvic organ function
Beyond Trigger Points: Neuromodulatory Targets
While trigger point deactivation is often cited as the primary mechanism, advanced practitioners now utilize dry needling to target peripheral nerves, spinal segmental reflex arcs, and viscerosomatic convergence zones relevant to pelvic dysfunction.
Key neuromodulatory targets include
- Obturator internus and levator ani — often hypertonic in cases of dyspareunia, pudendal neuralgia, or levator ani syndrome. Precise needling can reduce motor overactivity and pain referral.
- Sacral multifidi and paraspinals (S2–S4) — modulate pelvic floor reflex activity and impact bladder and bowel control.
- Gluteus maximus and piriformis — indirectly influence pudendal nerve path and pelvic floor muscle tone.
- Tibial nerve (posterior medial leg) — part of the sacral micturition reflex; targeted in dry needling or electroacupuncture for urge incontinence or bladder pain syndrome.
- Adductor group and iliopsoas — affect pelvic floor positioning and contribute to postural-driven pelvic dysfunction.
Additionally, cutaneous neurogenic zones, such as the sacral dermatomes and perineal region, may respond to superficial needling for neurosensory desensitization.
Application to Common Conditions
Pelvic Pain
Chronic pelvic pain involves peripheral tissue dysfunction, central sensitization, and autonomic dysregulation. Dry needling can:
- Interrupt pain-spasm-pain cycles
- Reduce afferent signaling from hyperactive pelvic muscles
- Decrease neuroinflammation via neuromodulation of spinal circuits
- Be combined with breathing techniques or down-training for improved autonomic regulation
Incontinence and Voiding Dysfunction
In urge incontinence, overactive detrusor activity may be linked to sacral reflex hyperexcitability. Dry needling — particularly of the posterior tibial nerve or S2–S4 paraspinals — may:
- Normalize afferent signaling to the pontine micturition center
- Restore motor balance between detrusor and external sphincter
- Improve pelvic floor muscle recruitment patterns when combined with EMG biofeedback
Sexual Pain or Dysfunction
In cases of vaginismus, vestibulodynia, or erectile dysfunction with pelvic myalgia, dry needling can:
- Reduce hypertonicity in the deep pelvic bowl (e.g., obturator internus, pubococcygeus)
- Increase local blood flow and nitric oxide release
- Support somatosensory reintegration, especially when layered with trauma-informed approaches
Integrating Dry Needling with Broader Neuromodulation Techniques
To fully leverage dry needling’s neuromodulatory capacity, it should be part of a multimodal care plan that may include:
- Electrical stimulation (e.g., intramuscular or percutaneous tibial nerve stimulation)
- Neurodynamic mobilization (e.g., pudendal nerve glide protocols)
- Manual therapy for visceral and connective tissue tension
- Somatic-based interventions for nervous system regulation and interoceptive awareness
- Behavioral strategies such as urge suppression techniques, pacing, and pelvic mapping
Safety and Clinical Reasoning
When applied near sensitive neurovascular and visceral structures, dry needling requires precise anatomical knowledge, informed consent, and advanced training. Ethical practice includes:
- Always using non-threatening, anatomically accurate language
- Avoiding direct needling of internal pelvic structures unless well-trained and permitted by state practice acts
- Employing real-time patient feedback and graded exposure techniques to minimize reactivity and optimize nervous system response
Clinical Pearls
- Always assess for central sensitization — if present, reduce peripheral input gradually and combine with education and graded sensory integration.
- Use ultrasound guidance or EMG if available for difficult-to-access muscles or when precision is paramount.
- Needle outside the pelvic floor (glutes, paraspinals, tibial nerve) when internal work is contraindicated, poorly tolerated, or not functionally required.
- Watch for signs of autonomic shift during or after treatment — sweating, dizziness, nausea — and manage with pacing and grounding techniques.
Dry needling is more than a mechanical intervention — it is a powerful interface with the nervous system. When skillfully applied, it opens new doors in the treatment of complex pelvic floor dysfunctions, especially those involving pain, inhibition, and neuromotor disruption. For advanced pelvic rehabilitation therapists, dry needling represents an opportunity not just to treat, but to modulate — to recalibrate the body’s own self-regulating systems toward a state of ease, control, and embodied safety.
Recommended Continuing Education:
Dry Needling and Pelvic Health: Foundational Concepts and Techniques — SOLD OUT
This course is the first in our pelvic health dry needling series. Designed for pelvic health practitioners, it teaches foundational dry needling techniques for treating pelvic floor and neuromusculoskeletal conditions such as lumbopelvic pain, incontinence, voiding issues, and sexual dysfunction. Participants will learn safe and effective needling for the female pelvic floor, as well as related areas including the spine, abdomen, pelvis, and hips. The course includes anatomy review, safety guidelines, plenty of lab practice, and clinical integration strategies.
Dry Needling and Pelvic Health Level 2: Advanced Concepts and Neuromodulation – August 2-3 in Duluth, MN
This advanced dry needling course offers a specialized approach to treating pelvic floor dysfunction related to pelvic pain, incontinence, voiding issues, and sexual pain. Participants will learn to apply dry needling techniques to both male and female pelvic floor muscles, as well as related areas like the spine, abdomen, pelvis, and hips. The course also covers neuromodulation concepts and techniques. Emphasis will be placed on anatomy review, safety, clinical reasoning, and hands-on lab practice to ensure confident and effective application in clinical settings.
Dry Needling and Pelvic Health: Pregnancy and Postpartum Considerations – August 23-24 in Lemont, IL
This course offers a specialized dry needling approach for treating neuromusculoskeletal conditions during pregnancy and postpartum. Topics include pelvic pain, carpal tunnel, plantar fasciitis, peripheral neuropathy, postural changes, and headaches. Participants will learn safe and effective needling techniques for the extremities, spine, and pelvic floor, with a focus on anatomy, safety, clinical application, and hands-on lab practice.
Resources:
- Dommerholt J, Fernández-de-las-Peñas C. Trigger Point Dry Needling: An Evidence and Clinical-Based Approach. 2nd ed. Churchill Livingstone; 2018.
- Kalichman L, Vulfsons S. "Dry Needling in the Management of Musculoskeletal Pain." J Am Board Fam Med. 2010;23(5):640–46.
- Young JL, Snodgrass SJ, Cleland JA, Rhon DI. “The Role of Dry Needling in Musculoskeletal Dysfunction: An Evidence-Informed Perspective.” Phys Ther. in Sport. 2019; 39:139–49.
- Asavasopon S, et al. “Brain Activity Associated with Pain in Female Pelvic Floor Muscles: A Functional MRI Study.” Neurourology and Urodynamics. 2014; 33(5):7.


As pelvic rehabilitation therapists, our role has traditionally focused on restoring continence, alleviating pain, and improving quality of life. Yet within athletic populations, pelvic floor dysfunction often presents in unique and nuanced ways—masked by high levels of conditioning, normalized symptoms, or misattributed pain patterns. As the bridge between performance and pelvic health, we are uniquely positioned to address these challenges.
In athletes, the pelvic floor must do more than support visceral structures or maintain continence. It plays an integral role in force transmission, lumbopelvic stability, breathing mechanics, and reflexive motor control. The demands of sport—sprinting, lifting, jumping, cutting—place high, repetitive loads on the core system, often revealing (or creating) dysfunctions in timing, tone, and coordination of the pelvic floor.
The athletic population requires a different lens: one that views the pelvic floor as a functional component of the kinetic chain and not in isolation.
Clinical Presentations: What We Commonly See
- Stress Urinary Incontinence (SUI) in High-Impact Sports: Female athletes, particularly in gymnastics, track, CrossFit, and volleyball, often experience SUI—yet many have strong pelvic floor muscles on MMT. The issue is frequently one of timing, coordination, or excessive tension rather than weakness. Screening for functional incontinence during movement (e.g., jumping or heavy lifting) is essential.
- Hypertonicity and Myofascial Pain: High-performing athletes often exhibit pelvic floor overactivity—either from compensatory stabilization or stress-related holding patterns. These individuals may present with deep hip pain, dyspareunia, tailbone pain, or abdominal discomfort. Common coexisting findings include labral pathology, SIJ dysfunction, and overuse injuries.
- Core Dysfunction and Lumbopelvic Instability: Poor load transfer across the pelvis, impaired breath mechanics, and delayed transversus or multifidus activation often coexist with pelvic floor dyscoordination. This population may present with chronic low back pain, hip impingement, or even sports hernia.
- Postpartum Athletes: Returning to sport postpartum brings unique challenges—diastasis recti, levator avulsion, prolapse, and deconditioning of core synergy. Pressure to return to performance prematurely can exacerbate dysfunction if pelvic rehabilitation is bypassed.
Assessment Considerations for the Athletic Client
In working with athletes, it’s critical to think beyond isolated internal examination and assess whole-system function:
- Breath and Pressure Management: Assess how the client regulates intra-abdominal pressure during dynamic tasks (e.g., lifting, landing, change of direction).
- Pelvic Floor Mobility and Control: Use internal and external assessments to evaluate both overactivity and under-recruitment, including timing during functional movement.
- Core Integration: Test synergistic recruitment of diaphragm, transversus abdominis, multifidus, and pelvic floor during anticipatory and reactive tasks.
- Functional Movement Screens: Incorporate squat mechanics, running gait analysis, lunge variations, and single-leg stability to evaluate force transfer and pelvic control under load.
- Load Testing: Progress assessments to mimic sport-specific demands—e.g., jumping with pelvic floor biofeedback, agility drills with breath cueing.
Treatment Priorities in Pelvic Rehab for Athletes
- Down-Training Before Strengthening: Many athletic clients do not need Kegels—they need to let go. Releasing hypertonic tissues, restoring breath, and retraining pelvic floor length-tension balance is often the starting point. Re-establishing proper sequencing of breath, pelvic floor, and deep core muscles is essential. Use dynamic cuing, load modulation, and real-time feedback (e.g., pressure biofeedback, US imaging) to reinforce neuromotor control.
- Myofascial and Manual Therapy: Trigger point release (levator ani, obturator internus), neural mobilization (pudendal nerve, obturator nerve), and SIJ or hip mobilizations are often necessary for full pelvic system mobility.
- Functional Reintegration: Rehabilitate pelvic floor activation in context—squatting, lifting, running, jumping. Train coordination across planes of motion, not just in supine or side-lying.
- Athlete-Specific Return-to-Play Criteria: Use objective metrics—continence during max effort, pelvic floor coordination under fatigue, breath control under load—to clear clients for return to sport. Consider incorporating pelvic floor testing into movement screens or performance evaluations.
Our Expanding Role
As pelvic rehab therapists, we are more than continence specialists—we are movement specialists. Within sports medicine, we bring a unique capacity to identify root causes of dysfunction that go unseen by traditional orthopedic approaches. Our collaboration with strength coaches, orthopedic PTs, sports MDs, and athletic trainers is critical in shaping a comprehensive, athlete-centered plan.
Pelvic rehabilitation is a performance tool. In the athletic population, our interventions can prevent injuries, improve performance, and support longevity in sport. By approaching the pelvic floor as a dynamic contributor to the kinetic chain, we can elevate the standard of care and advance our profession’s impact in sports medicine.
The Course Options
Athletes and Pelvic Rehabilitation remote course scheduled for July 26-27. In this course, Dr. Dischiavi covers evidence-based, immediately-applicable skills related to pelvic floor rehabilitation for the athlete, including treatment philosophies for the pelvis and pelvic floor, and global considerations of how these structures contribute to human movement. Topics include urinary incontinence, as well as the intricacies of athletic movement and how energy transference throughout the kinetic chain is crucial to the rehabilitation approach, injury prevention, and high performance. This course will also cover biomechanics behind human movement of the lumbopelvic-hip complex, so the participant will be able to prescribe effective and innovative therapeutic exercise programs. The connection of how pelvic rehab influences LE pathologies such as ACL, PFP, and chronic ankle instability will be covered. Although this class has a focus on athletes, these concepts of biomechanics and movement patterning are applicable to all patients in the clinic.
The Runner and Pelvic Health is a one-day, remote course scheduled for July 26, created and instructed by Aparna Rajagopal PT, MHS, WCS, PRPC, and Leeann Taptich DPT, SCS, MTC, CSCS. This course is designed to expand your knowledge of the pelvic floor in running athletes. Through lecture and labs by video and participation, participants will learn what normal and abnormal running mechanics are and how the muscles work simultaneously during running. This course includes advanced assessments to help diagnose the reason for movement dysfunction. All assessments can be easily integrated into a therapist's evaluation skill set. The course is applicable for patients who present with pelvic pain, incontinence, constipation, prolapse, postpartum, and lumbar pain.
All Upcoming Continuing Education Courses

Pelvic Function Level 1 - Satellite - Milwaukee WI - July 12 - 13 2025 - SOLD OUT
Jul 12 2025 - Jul 13 2025

Modalities and Pelvic Function - In-Person - Houston TX - July 12 - 13 2025
Jul 12 2025 - Jul 13 2025

Pelvic Function Level 1 - Satellite - Denver CO - July 12 - 13 2025 - SOLD OUT
Jul 12 2025 - Jul 13 2025




Pelvic Function Level 1 - Satellite - Des Moines IA - July 26 - 27 2025 - SOLD OUT
Jul 26 2025 - Jul 27 2025

Pelvic Function Level 1 - Satellite - Minneapolis MN - July 26 - 27 2025 - SOLD OUT
Jul 26 2025 - Jul 27 2025

Pelvic Function Level 1 - Satellite - Paso Robles CA - July 26 - 27 2025 - SOLD OUT
Jul 26 2025 - Jul 27 2025

Pelvic Function Level 1 - Satellite - St. Augustine FL - July 26 - 27 2025
Jul 26 2025 - Jul 27 2025

Pelvic Function Level 1 - Satellite - Virginia Beach VA - July 26 - 27 2025 - SOLD OUT
Jul 26 2025 - Jul 27 2025


Pelvic Function Level 1 - In-Person - Chicago IL - August 2 - 3 2025 - SOLD OUT
Aug 2 2025 - Aug 3 2025



Menopause Transitions and Pelvic Rehab - Remote Course - August 9 - 10 2025
Aug 9 2025 - Aug 10 2025









Pelvic Function Level 2C - Satellite - Palm Beach FL - August 16 - 17 2025
Aug 16 2025 - Aug 17 2025

Pelvic Function Level 2C - Satellite - New Orleans LA - August 16 - 17 2025
Aug 16 2025 - Aug 17 2025
Pelvic Function Level 2C - Satellite - Paso Robles CA - August 16 - 17 2025
Aug 16 2025 - Aug 17 2025


Pediatrics Level 1 - Treatment of Bowel and Bladder Disorders - Remote Course - August 23 - 24 2025
Aug 23 2025 - Aug 24 2025

Pelvic Function Level 1 - Satellite - Jacksonville FL - August 23 - 24 2025
Aug 23 2025 - Aug 24 2025

Pelvic Function Level 1 - Satellite - Chicago IL - August 23 - 24 2025 - SOLD OUT
Aug 23 2025 - Aug 24 2025


Rehabilitative Ultrasound Imaging Pelvic Health Satellite Lab Course - Self-Hosted - September 5 - 7 2025
Sep 5 2025 - Sep 7 2025
Rehabilitative Ultrasound: Orthopedic Topics Satellite Lab Course - Self-Hosted - September 5 - 6 2025
Sep 5 2025 - Sep 6 2025

Rehabilitative Ultrasound Imaging Pelvic Health Satellite Lab Course - Indianapolis IN - September 5 - 7 2025
Sep 5 2025 - Sep 7 2025
Rehabilitative Ultrasound: Orthopedic Topics Satellite Lab Course - Indianapolis IN - September 5 - 6 2025
Sep 5 2025 - Sep 6 2025
