Pelvic Rehab Report
The official Herman & Wallace blog. New blogs post every Friday on topics relating to the field of pelvic floor dysfunction.
Varicoceles are enlarged veins that occur in the scrotum. They can be common in adolescent boys and men, with an incidence rate of approximately 15%. Because up to 1/3 of men dealing with infertility have a varicocele, a repair of this venous herniation may be a first line treatment for male fertility. Varicoceles are sometimes referred to as feeling like a "bag of worms" due to the distended veins that coil through the area (the U.S. National Library of Medicine provides a useful illustration). Although varicoceles may be painless, they are thought to be symptomatic in up to 10% of men. Symptoms can be dull, aching, throbbing, and can worsen with physical activity. Conservative care includes scrotal support, limiting physical activity, and using anti-inflammatory medications.

Pelvic rehabilitation providers may work with a male patient who complains of scrotal pain, and who has a known diagnosis of a varicocele. If the patient is unsure of such a diagnosis, questioning the patient about prior discussions with his medical providers may reveal that he was told about “enlarged veins in the scrotum” or similar description. Visual inspection may reveal the tell-tale appearance of distended veins inside the scrotum, and palpation may reveal a significant difference among sides (unless both sides are involved of course.) Physical examination for a varicocele is usually completed in supine and standing positions and may be palpable with or without Valsalva maneuver. Keeping in mind that the differential diagnosis for pain in the scrotum can include medical conditions such as testicular torsion, epididymitis, inguinal hernia, testicular tumor, hydrocele, epididymal cyst, or sperm granuloma, patients who have complaints must see an appropriate medical provider to rule out such conditions. It is also possible for a patient’s condition to change or worsen if a period of time has passed, with communication with the referring provider recommended. Post-surgical complications that should also be considered are inguinal hernia repair for nerve entrapment or vasectomy.
Because of the nerves traveling in the same pathway as the involved veins, we can also consider the neural tension potentially created from the increased venous distension creating either (or both) compression and drag. Surgical options may be discussed by the medical provider, and these might include a microsurgical ligation or a varicolectomy. According to Park & Lee (2013) “A varicocelectomy should be considered in patients with no alleviation of their pain after conservative management, including resting, scrotal elevation, and nonsteroidal anti-inflammatory analgesics.” Conservative management is exactly where we can fit in as providers of pelvic rehabilitation. Including a condition such as a varicocele in our differential diagnosis and treating planning can further our success with patients.
Herman & Wallace offers it's popular Male Pelvic Floor Function, Dysfunction and Treatment course next month in Denver, CO. See you there!
References
Park, Y. W., & Lee, J. H. (2013). Preoperative predictors of varicocelectomy success in the treatment of testicular pain. The world journal of men's health, 31(1), 58-63.
Shridharani, A., Lockwood, G., & Sandlow, J. (2012). Varicocelectomy in the treatment of testicular pain: a review. Current Opinion in Urology, 22(6), 499-506.
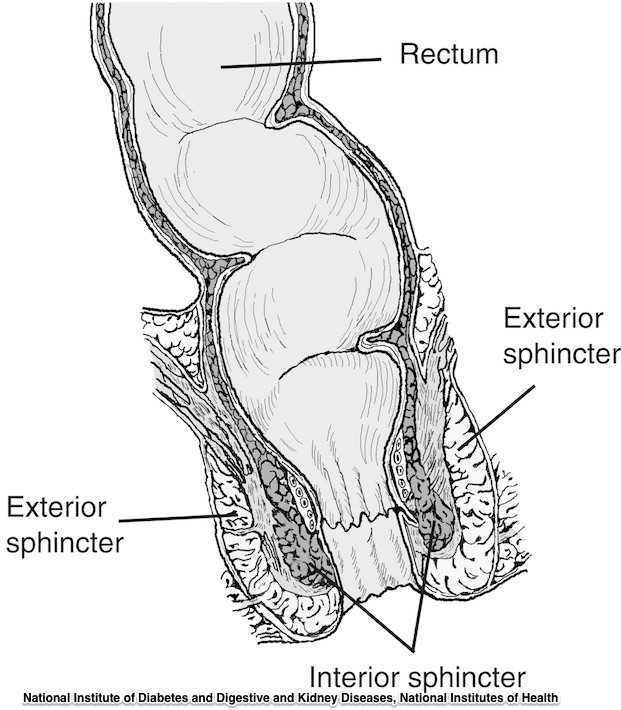
Guidelines for the management of 3rd and 4th degree tears were updated and published last month by The Royal College of Obstetricians & Gynaecologists. The purpose of the guidelines are to provide evidence-based guidelines on diagnosis, management and treatment of 3rd and 4th degree perineal tears. These types of tears are also referred to as obstetric anal sphincter injuries, or OASIS. The authors acknowledge an increased rate of reported anal sphincter injuries in England that may in part be due to increased awareness and detection of the issue. In terms of classification of anal sphincter injuries, the following is recommended (note the different levels at grade 3:
- 1st degree tear: injury to the perineal skin and/or the vaginal mucosa
- 2nd degree tear: injury to the perineum involving the perineal muscles but not involving the anal sphincter.
- 3rd degree tear: injury to the perineum involving the the anal sphincter complex
- Grade 3a tear: Less than 50% of the external anal sphincter (EAS) thickness is torn.
- Grade 3b tear: More than 50% of the EAS thickness is torn.
- Grade 3c tear: Both the EAS and the internal anal sphincter (OAS) are torn.
- 4th degree tear: Injury to the perineum involving the anal sphincter complex (EAS and IAS) and the anorectal mucosa.
Risk factors for anal injury are also outlined in the guidelines, although the authors point out that accurate prediction based on the risk factors is not reliable. The noted risk factors are as below:
- Asian ethnicity
- Nulliparity
- Birthweight greater than 4 kg (8.8 lb)
- Shoulder distocia
- Occipito-posterior position
- Prolonged 2nd stage labor
- Instrumented delivery
Recommendations worth noting include Level A evidence that warm compression during the 2nd stage of labor reduces the risk of OASIS. A noted best practice recommendation is that “Women should be advised that physiotherapy following repair of OASIS could be beneficial.” Guidelines such as these from The Royal College of Obstetricians & Gynaecologists can help in creating common language and in making recommendations that improve communication and expectations between patients and providers.
If you are interested in learning more about anal tears, Herman & Wallace offers several courses which cover the topic. For postpartum care specifically, check out Care of the Postpartum Patient.
The research on pelvic pain and specifically on sexual dysfunction has focused on heterosexual women, leaving a large gap in the clinically-based evidence. A study published last year in the Journal of Sex & Marital Therapy aimed to narrow this gap by studying the characteristics of vulvar pain in women in a variety of relationships. The associations between qualities such as love and communication were evaluated in relation to the participants' perceptions of how pain influenced their relationships. Within the research report, the authors establish that pelvic pain commonly causes pain and limitation with sexual function, and that queer women (defined in their work as women who identify as something other than heterosexual) also experience pain with sexual function.
"Of the 839 women, 31% reported genital pain, with 12% of the women with genital pain in a same-sex relationship, 67% in a mixed-sex relationship, and 21% being single"
The women in the study provided information about demographics, experiences of genital pain and pain characteristics. They completed surveys including the Dyadic Trust Scale (measures trust in a close relationship), the Rubin Love Scale (assesses level of romantic love), and the Communication Subscale of Evaluation and Nurturing Relationship Issues, Communication and Happiness Marital Satisfaction Scale (measures level of communication). Participants' average age was 25, and of the 77% who were in a relationship, most (60%) were in a mixed-sex relationship. Average length of relationships was 3 years, with nearly 84% of the women being white with some level of higher education.
Of the 839 women, 31% reported genital pain, with 12% of the women with genital pain in a same-sex relationship, 67% in a mixed-sex relationship, and 21% being single. Of the 260 women reporting genital pain, 39% identified as heterosexual, 15% identified as lesbian, and 46% identified as bisexual. The most common pain locations reported were inside the vagina (48%), in the pelvis or abdomen (45%), at the vaginal opening (39%), and 21% of the women reported global vulvar pain. From the data, the authors also report that women in same-sex relationships were likely to report that tampon insertion was painful.
The authors point out that challenges to healing for women who identify outside of heterosexual are many, and can include:
- homonegativity and heterosexism at a medical provider's office
- failure to disclose sexual identity due to fear of negative interaction
- fear that a symptom is linked to a sexual practice
- being in an unsupportive relationship or having poor adjustment within relationship
The limited research on sexual pain in women in same sex relationships has highlighted strengths within the relationships as well. Women in same sex relationships have been noted to have more effective communications skills, which may in turn foster better understanding of conditions such as pelvic pain. The authors concluded that while the characteristics of vulvar pain were similar across groups, there was a difference in the perception of pain impact on relationships. Better communication for same-sex couples and more love for mixed-sex couples was positively associated with impact on relationship. Of the women reporting pain, nearly half of the participants indicated that the pain negatively impacted their relationship in general, and 64% reported that the pain interfered with sexual health.
This type of research provides insight for pelvic rehabilitation clinicians and adds to our data base of considerations when working with women. The truth is that most of us were not provided adequate training in how to evaluate and manage issues of sexual health, nor were we provided with the means to value our own sexuality as a normal and healthy part of being. This lack requires education to fill in our own gaps, so that we can be of best service to our patients. If we are able to be present and nonjudgmental, our patients can in turn share openly and provide information that can direct best care. Holly Herman, co-founder of the Pelvic Rehabilitation Institute, offers a 2-day course in Sexual Medicine, so that providers can learn more about healthy sexuality as well as how to dialog with our patients.
Michelle Lyons is instructor of "Oncology and the Female Pelvic Floor: Female Reproductive and Gynecologic Cancers", among other Herman & Wallace courses. We thought you might like to hear her expert analysis of current research going on in the field of gynecologic oncology, and the benefits therapeutic yoga can have on patient rehabilitation. Take it away, Michelle!

More than 65,000 women are diagnosed with gynecologic cancers (vulvar, vaginal, cervical, ovarian, endometrial) in the United States each year (Sohl et al 2012). Treatment options for these women include surgery, chemotherapy, radiation and hormone therapy – all of which have the potential to have local, regional and global effects on a woman’s body. The pelvic rehab specialist is in a unique position to hugely improve quality of life issues for these women – dealing with issues directly associated with pelvic health (urinary, sexual and bowel function and dysfunction) as well as more global issues such as bone health, peripheral neuropathies and musculoskeletal dysfunctions.
Yoga has enormous potential as a therapeutic tool for gynecologic cancer survivors and as exercise prescription experts, we can add yoga as a multi-purpose tool to our skill-set.
Empirical research on therapeutic yoga has been ongoing for several decades, including several recent studies conducted with cancer patients and survivors. Although most of the research looking at the benefits of yoga for cancer survivors has been done in the context of breast and prostate cancers, we can safely extrapolate many of the benefits associated with oncology rehab yoga, including its immediately obvious ability to improve flexibility, strength, balance, but also the impact yoga can have on decreasing inflammation, improving sleep and raising quality of life scores in pelvic cancer survivors.
Recent papers by Dewhirst et al showed how moderate exercise can improve the efficacy of chemotherapy and radiation by decreasing tumour hypoxia – they also discovered that this may limit metastatic aggression.
We also know that exercise can be potent medicine when it comes to dealing with the effects of cancer treatments, especially fatigue, bone health and cardiovascular function, which may disrupt return to exercise (Kerry et al 2005). But pelvic cancer patients may face extra barriers when it comes to returning to exercise, such as pelvic pain and concerns about continence, as well as diminished flexibility, balance and strength. But as Blaney et al concluded in their 2013 paper ‘…however, the main barriers reported were those that had the potential to be alleviated by exercise.’ And in my opinion, this can be achieved by integrating yoga into our pelvic oncology rehab programs.
These recent and exciting research findings have encouraged me to add a therapeutic yoga lab session to my Oncology & the Pelvic Floor course, which I will be teaching in NY next month. This is the last chance to catch this course stateside this year so I hope you will join me in White Plains to explore the many ways we can make a serious impact on pelvic cancer survivorship (Bring your yoga mat!)
References:
Psychooncology. 2013 Jan;22(1):186-94.
Cancer survivors' exercise barriers, facilitators and preferences in the context of fatigue, quality of life and physical activity participation: a questionnaire-survey. Blaney JM1, Lowe-Strong A, Rankin-Watt J, Campbell A, Gracey JH.
Annals of Behavioral Medicine
April 2005, Volume 29, Issue 2, pp 147-153
A Longitudinal Study of Exercise Barriers in Colorectal Cancer Survivors Participating in a Randomized Controlled Trial
Kerry S. Courneya Ph.D., Christine M. Friedenreich Ph.D., H. Arthur Quinney Ph.D., Anthony L. A. Fields M.D., Lee W. Jones Ph.D., Jeffrey K. H. Vallance M.A., Adrian S. Fairey M.Sc.
JNCI J Natl Canc
Allison S. Betof, Christopher D. Lascola, Douglas H. Weitzel, Chelsea D. Landon, Peter M. Scarbrough, Gayathri R. Devi, Gregory M. Palmer, Lee W. Jones, and Mark W. Dewhirst
Modulation of Murine Breast Tumor Vascularity, Hypoxia, and Chemotherapeutic Response by Exercise
Pelvic rehabilitation providers commonly treat a variety of conditions associated with peripartum pelvic girdle dysfunction. This list of conditions includes coccyx pain, and a recent study aimed to identify risk factors which may lead to coccyx pain in the postpartum period. Dr. Jean-Yves Maigne, who is well known for providing foundational research on the topic of coccyx pain, and colleagues completed a case series of 57 postpartum women presenting to a specialty coccydynia clinic. Dynamic x-rays were taken to assess mobility of the coccyx, and data about delivery methods were collected. (A control group of 192 women were comprised of women who also presented to the clinic but who had coccyx pain from other causes.)
The authors found that the women reported immediate postpartum pain in the coccyx with sitting. Instrumentation was a common finding in regards to the patients’ deliveries. 50.8% of the deliveries utilized forceps while 7% were vacuum-assisted. An additional 12.3% of the deliveries were spontaneous and were described as “difficult.” A subluxation of the coccyx was observed in 44% of the women who developed coccyx pain after childbirth as compared to 17% of the controls. A fractured coccyx occurred in 5.3 % of the women. Body mass index (BMI) of more than 27 and having 2 or more vaginal deliveries was also associated with a higher prevalence of a subluxation of the coccyx.
Being unable to sit comfortably following childbirth could make a new parent’s life very difficult with limitations in activities such as sitting to feed the baby. Socially, being unable to sit comfortably can also limit many activities. The women in this study reported immediate tailbone pain with sitting, which can alert providers to a condition requiring both immediate and follow-up attention. Risk factors such as having a difficult delivery or use of forceps may also signal a patient history that may lead to coccyx pain.
If you are interested in learning more about managing coccyx pain, join Lila Abbate at Coccyx Pain Evaluation and Treatment in Bay Shore, NY on October 25-26! You may also be interested to learn more about treating patients during the postpartum period, in which case Care of the Postpartum Patient is right up your alley!

Today we are fortunate to hear from Barbara S. Rabin MSPT ATC PYTc, owner and practitioner at Holistic Physical Therapy in Gates Mills, OH. Barbara has more than 20 years of experience in orthopedic rehabilitation. Her perspective as an athletic trainer and orthopedic therapist highlights the many approaches practitioners can take when working with pelvic rehabilitation patients.
"We were reminded how all the muscles of the hip are intricately integrated into the pelvic floor and one can’t ignore the influence and interaction they have on each other."
My physical therapy career has been in the world of outpatient orthopedics and sports medicine. While in physical therapy graduate school I became a nationally certified athletic trainer, and most of my post graduate CEU’s have been in the orthopedic and sports medicine arena.
Stepping Outside the Comfort Zone
As an orthopedic PT, it was “safe” to study the pelvic girdle when I took Richard Jackson’s continuing education course in 1994 because it focused on muscles, ligaments, bones and nerves. However, I was leaving “safe territory” when I took Janet Hulme’s course, “Beyond Kegels: Evaluation and Treatment of Pelvic Muscle Dysfunction and Incontinence” in 1998. Long ago, back in gross anatomy lab in physical therapy school, we barely looked at the pelvic floor contents. Yes, we identified the digestive system but basically ignored all of the rest. Our mission was mostly to learn the muscles, ligaments, bones and nerves. After Janet Hulme’s course, I tried to offer incontinence rehabilitation at my place of employment at the time, but the idea was quickly dismissed. However, I am very glad to say that pelvic floor rehab is now commonly offered at most major hospitals and many clinics.
I continued my education of the pelvis and hip in several other courses and especially enjoyed one I attended last year called, "Extra-Articular Pelvic and Hip Labrum Injury: Differential Diagnosis and Integrative Management" by the Herman & Wallace Pelvic Rehabilitation Institute and taught by Ginger Garner PT ATC PYT. We were reminded how all the muscles of the hip are intricately integrated into the pelvic floor and one can’t ignore the influence and interaction they have on each other.
I was intrigued and wanted to learn more about the pelvic floor. I got another opportunity when I most recently attended an intimidating course for an “orthopedic sports medicine physical therapist” called, “Mobilization of Visceral Fascia for the Treatment of Pelvic Dysfunction - Level 1: The Urinary System” taught by Ramona Horton, MPT. I learned that externally mobilizing the bladder can often increase hip extension. Here was a combining of the fascial, pelvic floor, and orthopedic worlds!
Myofascial Release and Other Manual Therapy
I learned several manual therapy techniques in courses, and I took the best out of many but never specialized. As of late, I have been gladly drawn into the world of John F Barnes myofasical release. Studying and working with the fascia coincides with my holistic approach of rehabilitation, since the fascia is intricately woven throughout our body. The fascia was another thing we ignored in gross anatomy lab in physical therapy school. It was cut to move it out of the way so we could “get to the important stuff.” Even in that dead and embalmed state, the fascia was fascinating. It was strong and flexible at the same time. Now, with the advent of micro discography of the fascia by Dr. Jean-Claude Guimberteau (http://www.guimberteau-jc-md.com/en/biographie.php) we can view fascia in its live state and we can really see the phenomenal structure that it truly is.
Incorporating Yoga into Rehabilitation Practices
About eight years ago I took my first yoga class. I thought I was a conditioned athlete as a lifelong runner but I was humbled as I could not even balance on one leg for a minute. I noticed the physical and emotional benefits in myself and wanted to include yoga in the treatment of my patients. I had a patient who had physical issues from an eating disorder and needed supervision to exercise. I thought to myself that what she needed was not physical therapy but possibly meditation and relaxation. Even though I didn’t learn those techniques in PT school, I felt that I should be able to offer them to my patients. With one yoga class under my belt, in 2007, I entered into a 200 hour teacher training with Marni Task studying her combination of Jivamukti and Anusara yoga. I further continued my yoga training in 2011 with Ginger Garner PT, ATC, PYT of Professional Yoga Therapy Studies (http://proyogatherapy.org). Her school of medical yoga training, was just what I was looking for to merge my worlds of physical therapy and yoga.
Instead of looking at our patients as “pieces and parts,” referring to them as “the knee or the shoulder patient,” it is so important to see them as a whole. As an orthopedic PT I need to recognize that patients have not only a physical side of muscles, ligaments, bones and nerves, but other parts too that make them a whole person. Most likely I won’t specialize in pelvic pain or woman’s health but it is so important for me to be knowledgeable about this field to be the most effective therapist. In addition, it’s important to also go beyond the physical aspect and recognize patient’s psycho-emotional-social, spiritual, energetic, and intellectual aspects of their beings. Optimal health is achieved by recognizing and addressing all aspects of a patient.
And on that note, I’m going to continue merging all of my worlds of fascia, pelvic floor, orthopedics, and yoga, to address all the components of well-being, as I attend an upcoming course offered by Herman and Wallace called, Yoga for Pelvic Pain this month in Cleveland, Ohio.
Do you have a burning question about pelvic rehabilitation? Herman & Wallace faculty member Michelle Lyons will be happy to help! The Pelvic Rehab Report will be conducting an interview with Michelle and we are inviting you to submit your questions. Head over to www.hermanwallace.com/michelle-lyons-question-and-answer if you are curious to hear about what it's like treating pelvic pain patients, some of Michelle's experiences practicing abroad, teaching courses to practitioners, or about her favorite pasta sauce! We will take the top 5 or 10 questions and put Michelle through the ringer.
Michelle Lyons PT, MISCP, is a graduate of University College Dublin, Ireland, with over eighteen years experience working in women's health. A firm believer in integrative healthcare, she incorporates therapeutic pilates, yoga and lifestyle advice into her treatment protocols.
Michelle has appeared in local newspapers, radio and television programs speaking on women's health issues. She has presented programs in Ireland, Canada and the U.S. including The Wise Woman weekend, The International Herbal Symposium and The New England Women's Herbal Conference and for the Irish Society of Chartered Physiotherapists.
Michelle has written several courses which she instructs with Herman & Wallace. The list includes Menopause Rehabilitation and Symptom Management, Special Topics in Women's Health: Endometriosis, Infertilty and Hysterectomy, Oncology and the Female Pelvic Floor: Female Reproductive and Gynecologic Cancers, and Oncology and the Male Pelvic Floor: Male Reproductive, Bladder, and Colorectal Cancers.

What are you saying when giving directions to men during pelvic floor muscle training, and how do those instructions affect the effectiveness of a contraction? These questions are tackled in a study that is very interesting to therapists working in pelvic dysfunction. 15 healthy men ages 28-44 (with no prior training in pelvic floor training) were instructed to complete a submaximal effort pelvic muscle contraction. Tools utilized to acquire data in the study include those below:
| Assessment tool | Measuring |
| Transperineal ultrasound | displacement of pelvic floor landmarks |
| Surface EMG (electromyography) | abdominal, anal sphincter muscle activation |
| Nasogastric transducer | intra-abdominal pressure (IAP) |
| Fine wire electromyography (3 participants only) | puborectalis, bulbocavernosus muscles |
Participants sat upright on a plinth (backrest reclined at ~20 degrees with their knees extended). Directions for the submaximal efforts were given by telling the men to produce a level 3/10 effort with 10 being a maximal contraction. The men were instructed to hold the contraction for 3 seconds, and they were given 10 seconds rest between each of the 4 contractions using different verbal cues. (This series of 4 contractions was repeated with randomization for verbal cues, with a 2 minute rest in-between.) Verbal instructions were intended to target specific contractile tissues as described below- some of this theory could be validated via the fine wire EMG.
| Verbal cue | Targeting |
| "tighten around the anus" | anal sphincter |
| "elevate the bladder" | puborectalis |
| "shorten the penis" | striated urethral sphincter |
| "stop the flow of urine" | striated urethral sphincter, puborectalis |
Displacement, IAP, and abdominal/anal EMG were compared for the different verbal instructions. The greatest dorsal displacement of the mid-urethra and striated urethral sphincter activity was noted with the instruction to "shorten the penis." "Elevate the bladder" encouraged the greatest increase in abdominal EMG and IAP, while "tighten around the anus" induced the greatest anal sphincter activity. Displacement of pelvic landmarks correlated with EMG readings of the muscles thought to produce the targeted movement. The authors conclude that the therapist's choice of verbal instructions can influence the muscle activation and urethral movement in men. They suggest "shorten the penis" and "stop the flow of urine" for optimal activation of the striated urethral sphincter. They also point out the fact that by using the fine wire EMG and correlating muscle activation to observations with the transperineal ultrasound, the study validates the use of the less invasive method. If you are ready to jump into more education about male pelvic rehabilitation, join us in Denver in early August, or Seattle in November.
Today we get the opportunity to hear from Herman & Wallace faculty member Elizabeth Hampton PT, WCS, BCIA-PMB! Elizabeth has been kind enough to offer her insights about the diagnosis of pelvic rehabilitation patients. Join Elizabeth at Finding the Driver in Pelvic Pain this November in Houston, TX in order to learn evaluation tools for complex pelvic pain clients!
 Having taught for Herman and Wallace since 2006, I have a few observations that have been consistent over the years. Clinicians want their clients to get better, so much so that they are ready to jump in to treatment before having a solid problem list and validated findings. I can understand this: after a 3 day course we have clients Monday morning at 8 a.m. who have been waiting for us to take this course so we can get them better! We had better be smart ASAP! But what do we do when we are treating symptoms rather than understanding the primary, secondary and tertiary factors in their condition?
Having taught for Herman and Wallace since 2006, I have a few observations that have been consistent over the years. Clinicians want their clients to get better, so much so that they are ready to jump in to treatment before having a solid problem list and validated findings. I can understand this: after a 3 day course we have clients Monday morning at 8 a.m. who have been waiting for us to take this course so we can get them better! We had better be smart ASAP! But what do we do when we are treating symptoms rather than understanding the primary, secondary and tertiary factors in their condition?
Finding the Driver in Pelvic Pain is a course that is a foundational first step in screening the pelvic pain client. It is a great place to start. I developed the course because there was no evidence based comprehensive factors that had been established as fundamentals for screening a pelvic pain client.
The other thing I have learned after teaching Pelvic Floor Function, Dysfunction, & Treatment – Level 2B for 9 years is that the majority of clinicians who take this intermediate level course cannot perform a precise vulvar and intrapelvic muscle mapping assessment. Close your eyes and pretend you are mapping a client’s left iliococcygeus: can you place your finger in the proper orientation and know 100% you would be palpating it? Indeed, this takes training and repetition. Internal pelvic floor muscle mapping is a key part of the Finding the Driver screening system.
What do you do when you have a pelvic pain client on your schedule and a 45-60 minute slot? How do you screen findings and get the plan of care within such a short period of time? Finding the Driver is a comprehensive pelvic floor and musculoskeletal screening to rule in or rule out drivers of the pain from all sources including spine, pelvic ring, neural entrapment, intra-articular hip, load transfer, biomechanics and motor control. There is a clear flow to the screening process and an emphasis on how to organize that information, as we know with pelvic pain, it is the copious amount of information that is the challenge. We have two case studies with either participants or clients of a local Physical Therapist who come in and we go through the entire screen, prioritize treatment and provide that treatment during the course. The participants walk away with clear clinical reasoning for their treatment and prioritization of treatment as primary, secondary, and so on. The goal of the course is to help the clinician sort through the extraordinary amount of information we gather on our pelvic pain client and organize it in a way that we can explain to the client as well as create our plan of care. Treatment is not linear, as we are frequently treating many aspects at the same time. However being able to organize the information is key in designing that plan of care. For example, with a prone knee bend that reproduces labial pain, we find that the genitofemoral nerve is causing referred pain. However that referral may be due to constipation, irritable bowel, inguinal entrapment due to hernia surgery, intra-abdominal adhesions due to endometriosis, osteitis pubis or facilitated segment at the upper lumbar spine. How do we tease that out? How do you sequence nerve glide, visceral work, soft tissue mobilization, joint mobilization and dietary components for colonic motility? The treatment with all of those components are very different indeed. Finding the Driver is a hands on course with systematic screening tools and, with case studies, we go through treatments appropriate to that client. The focus is on what we, as physical therapists, can do to understand the drivers.
At the last Finding the Driver course in Milwaukee, WI, we had two case studies in pelvic pain. One client reported chronic psoas and adductor tightness with deep left sided pelvic pain. As a professional aerialist, she was extraordinarily flexible and demonstrated positions of tightness that concerned her, which included lateral splits with her hips in slight horizontal abduction and extension (yes, yikes!) When she reported that her adductor felt tight in this position, I explained it was because it was trying to keep her leg attached to her body! She was 9/9 on the Beighton scale and had severe multidirectional instability in her hips, impaired load transfer through her pelvis, respiratory dysfunction with efforts at pelvic floor and transverse abdominis contraction, as well as repeated choice of activities that were profoundly provoking. Interestingly, she was better at load transfer during handstands (bilateral or unilateral) vs. in standing and we discussed her course of treatment addressing the primary, secondary and tertiary aspects of her condition. Another client had severe labial pain, and despite multiple abdominal and intravaginal surgeries, her symptom onset was 4 months prior. She certainly had visceral, postural, joint restrictions, movement dysfunction and many other factors. But her primary driver was a labral tear in her hip and she needed surgery. After surgery, her pain was 100% resolved and in her post op rehab, the other factors could be addressed.
It is safe to say that it can be difficult to perform a comprehensive screen in 45-60 minutes on ALL clients. We all know that many of our clients need to tell their story and because of fear or previous negative history, we may choose as clinicians how to spend that session to best honor the needs of the client. That being said, Finding the Driver is a course which provides a solid start in differential diagnosis so you can drill down into more specifics on subsequent visits.
Visceral therapy is increasingly used by manual therapists, and research continues to emerge that attempts to explain the underlying mechanisms of the techniques. A study published in the Journal of Bodywork & Movement Therapies in 2012 reports on the effects of visceral therapy on pressure pain thresholds. Osteopathic visceral mobilization was applied to the sigmoid colon in 15 asymptomatic subjects. Pressure pain thresholds were measured at the L1 paraspinal muscles and 1st dorsal interossei before and after intervention. Pressure pain thresholds at the level assessed improved significantly immediately following the visceral mobilization. The effect was not found to be systemic. Hypoalgesia, therefore, may be a mechanism by which visceral mobilization affects patients who are treated with this technique.
Another research study that aimed to assess the effects of visceral manipulation (VM) on low back pain found that the addition of VM to a standard physical therapy treatment approach did not provide short term benefits. However, when the 64 patients were reassessed at 2, 6, and 52 weeks following treatment, the patients in the group with visceral manipulation were found to have less pain at 52 weeks. The patients were randomized into 2 equal groups and were provided physical therapy plus a placebo visceral treatment or a visceral treatment in addition to physical therapy. The authors propose that there may be long-term benefits of including visceral therapy in rehabilitation approaches.
If you would like to learn more about visceral techniques as well as theory and clinical application, check out the schedules for Ramona Horton's Visceral Mobilization 1 (VM1): The Urologic System, and Visceral Mobilization 2 (VM2): The Reproductive System. The first opportunity to take VM1 is in November in Salt Lake City and VM2 is scheduled in September in Ohio.
By accepting you will be accessing a service provided by a third-party external to https://www.hermanwallace.com/
All Upcoming Continuing Education Courses



Pelvic Function Level 1 - In-Person - Greensboro NC - June 7 - 8 2025 - SOLD OUT
Jun 7 2025 - Jun 8 2025

Nutrition Perspectives for the Pelvic Rehab Therapist - Remote Course - June 7 - 8 2025
Jun 7 2025 - Jun 8 2025





Pelvic Function Level 1 - Satellite - Torrance CA - June 14 - 15 2025 - SOLD OUT
Jun 14 2025 - Jun 15 2025

Pelvic Function Level 1 - Satellite - Long Beach CA - June 14 - 15 2025 - SOLD OUT
Jun 14 2025 - Jun 15 2025

Pelvic Function Level 1 - Satellite - Woodbury NY - June 14 - 15 2025 - SOLD OUT
Jun 14 2025 - Jun 15 2025


Pelvic Function Level 1 - Satellite - New York NY - June 14 - 15 2025 - SOLD OUT
Jun 14 2025 - Jun 15 2025

Pain Science for the Chronic Pelvic Pain Population - Remote Course - June 21 - 22 2025
Jun 21 2025 - Jun 22 2025

Dry Needling and Pelvic Health - In-Person - Atlanta GA - June 21 - 22 2025 - SOLD OUT
Jun 21 2025 - Jun 22 2025



Mobilization of Visceral Fascia - Gastrointestinal - Satellite Lab Course - St. Petersburg FL - June 27 - 29 2025
Jun 27 2025 - Jun 29 2025

Mobilization of Visceral Fascia - Gastrointestinal - Satellite Lab Course - Self-Hosted - Jun 27 - 29 2025
Jun 27 2025 - Jun 29 2025

Mobilization of Visceral Fascia - Gastrointestinal - Satellite Lab Course - Sellersville PA - June 27 - 29 2025
Jun 27 2025 - Jun 29 2025

Mobilization of Visceral Fascia - Gastrointestinal - Satellite Lab Course - Milwaukee WI - June 27 - 29 2025
Jun 27 2025 - Jun 29 2025

Mobilization of Visceral Fascia - Gastrointestinal - Satellite Lab Course - Medford OR - June 27 - 29 2025
Jun 27 2025 - Jun 29 2025

Mobilization of Visceral Fascia - Gastrointestinal - Satellite Lab Course - Bartlett IL - June 27 - 29 2025
Jun 27 2025 - Jun 29 2025

Mobilization of Visceral Fascia - Gastrointestinal - Satellite Lab Course - Cedar Knolls NJ - June 27 - 29 2025
Jun 27 2025 - Jun 29 2025

Mobilization of Visceral Fascia - Gastrointestinal - Satellite Lab Course - Marysville OH - June 27 - 29 2025
Jun 27 2025 - Jun 29 2025

Mobilization of Visceral Fascia - Gastrointestinal - Satellite Lab Course - New Orleans LA - June 27 - 29 2025
Jun 27 2025 - Jun 29 2025

Mobilization of Visceral Fascia - Gastrointestinal - Satellite Lab Course - Albany NY - June 27 - 29 2025
Jun 27 2025 - Jun 29 2025

Mobilization of Visceral Fascia - Gastrointestinal - Satellite Lab Cource - Amherst OH - June 27 - 29 2025
Jun 27 2025 - Jun 29 2025

Mobilization of Visceral Fascia - Gastrointestinal - Satellite Lab Cource - Paso Robles CA - June 27 - 29 2025
Jun 27 2025 - Jun 29 2025

Mobilization of Visceral Fascia - Gastrointestinal - Satellite Lab Course - Detroit MI - June 27 - 29 2025
Jun 27 2025 - Jun 29 2025



Pelvic Function Level 1 - Satellite - Tampa FL - June 28 - 29 2025 - SOLD OUT
Jun 28 2025 - Jun 29 2025


Pelvic Function Level 1 - Satellite - Waco TX - June 28 - 29 2025 - SOLD OUT
Jun 28 2025 - Jun 29 2025



Pelvic Function Level 1 - Satellite - Milwaukee WI - July 12 - 13 2025 - SOLD OUT
Jul 12 2025 - Jul 13 2025

Modalities and Pelvic Function - In-Person - Houston TX - July 12 - 13 2025
Jul 12 2025 - Jul 13 2025
Pelvic Function Level 1 - Satellite - Denver CO - July 12 - 13 2025 - SOLD OUT
Jul 12 2025 - Jul 13 2025

Pelvic Function Level 2B - Satellite - Sellersville PA - July 19 - 20 2025
Jul 19 2025 - Jul 20 2025