Pelvic Rehab Report
The official Herman & Wallace blog. New blogs post every Friday on topics relating to the field of pelvic floor dysfunction.
Recently in the Pelvic Rehab Report blog we discussed the beneficial role of pelvic rehabilitation for symptoms of dysmenorrhea. Additional research was published this year that supports the use of pranayama for improving quality of life and pain in girls with primary dysmenorrhea. Breathing within yoga studies is a rich field, with well-defined variations in stages and kinds of breathing, techniques and postures, and use of different hand positions and breathing through the nostrils and/or mouth. The Oxford online dictionary defines pranayama as a practice coming from Hindu yoga and related to regulating the breath through specific techniques.

In the study, the practice of both slow pranayama (Nadi Shodhan) and fast pranayama (Kapalbhati) was instructed to the women to be completed in the mornings on an empty stomach for 10 minutes per day. Ninety unmarried young women (ages 18-25) diagnosed with primary dysmenorrhea were randomly and equally assigned to either Group A (slow pranayama) or Group B (fast pranayama). Outcomes included the Moos menstrual distress questionnaire (MMDQ), numerical pain rating pain scale, a quality of life scale "by American chronic pain association" and the assessments were administered at baseline, after the first menstrual cycle, and after the second menstrual cycle. To read more details about the methods and results, the full article can be accessed here.
Prior and recent research has also studied the effects of similar breathing techniques on cognitive functions in healthy adults and also on perceived stress and cardiovascular parameters in young healthcare students. While it may not be new to compare fast and slow pranayama techniques with health conditions, this is the first study to address pranayama's effects on symptoms of dysmenorrhea. The authors conclude that practicing slow pranayama compared to fast pranayama improved quality of life and pain scores related to dysmenorrhea. Furthermore, the authors suggest that because pranayama can decrease absenteeism and stress levels, the practice should be implemented in college students to improve quality of life.
If you are looking to learn more about pranayama and other methods of self-management of conditions including, but certainly not limited to, dysmenorrhea, come to the city-New York City- next month for Meditation for Patients and Providers instructed by faculty member Nari Clemons. It's sure to be hot in the city, so chill out indoors with Nari, and hang out at night with your new favorite colleagues that you'll meet. A benefit of this course is that not only can you learn to care better for your patients, but also for yourselves, and you deserve it.

Today we present Part II of Michelle Lyons' discussion on sex after gynecologic cancer. Michelle will be teaching a course on this topic in White Plains in August!
In Part One of this blog, I looked at the sexual health issues women face after gynecologic cancer. In Part Two, I want to explore different treatment options that we as pelvic rehab specialists can employ to help address the many implications of cancer and cancer treatment
Treatment for gynecologic cancers, including vulvar, vaginal, cervical, endometrial and ovarian cancers, may include surgery, radiation therapy, chemotherapy, and/or hormonal therapy. We know that any of these approaches can have an adverse effect on the pelvic floor, as well as systemic effects on a woman’s body. Issues can include pain, fibrosis, scar tissue adhesions, diminished flexibility, fatigue and feeling fatigued and unwell. The effects on body image should not be under-estimated either. In their paper ‘Sexual functioning among breast cancer, gynecologic cancer, and healthy women’, Anderson & Jochimsen explore how ‘…body-image disruption may be a prevalent problem for gynecologic cancer patients…more so than for breast cancer patients’. The judicious use of manual therapy and local and global exercise prescription may be excellent pathways for a women to re-integrate with her body.
Many women will have to learn to care for a new colostomy or how to catheterize a continent urostomy. A woman who has had a vulvectomy will need sensitive counselling to understand that she can still respond sexually. Patients who have had a vaginectomy with reconstruction as part of a pelvic exenteration will need extensive rehab to help them achieve successful sexual functioning. We as pelvic rehab practitioners are in a uniquely privileged position – not only can we ask the questions and discuss the options but we are licensed to be ‘hands on’ professionals, using our core skills of manual therapy, bespoke exercise advice and educating our patients about a range of issues from the correct usage of lubricants, dilators, sexual ergonomics and brain/pain science. I am in the habit of describing pelvic rehab as the best specialty in physical therapy but I think this is especially true when it comes to the junction of oncology and pelvic health. This is where we can integrate our knowledge of neuro-science, orthopaedics, the lymphatic system and pelvic health to deal with the effects of pelvic cancers and their treatment.
In Farmer et al’s 2014 paper, ‘Pain Reduces Sexual Motivation in Female But Not Male Mice’ , the authors found that ‘Pain from inflammation greatly reduced sexual motivation in female mice in heat -- but had no such effect on male mice’. Unfortunately ongoing pelvic pain is a common sequela of treatment for gynecologic cancers – reasons ranging from post-operative adhesions, post-radiation fibrosis or vaginal stenosis or genital lymphedema. It is also worth bearing in mind the ‘rare but real’ scenario of pudendal neuralgia following pelvic radiation, as discussed by Elahi in his 2013 article ‘Pudendal entrapment neuropathy: a rare complication of pelvic radiation therapy.’
The good news is that we have much to offer. Yang in 2012 (‘Effect of a pelvic floor muscle training program on gynecologic cancer survivors with pelvic floor dysfunction: A randomized controlled trial’) showed that pelvic rehab improved overall pelvic floor function, sexual functioning and QoL measures for gynecological cancer patients. Yang’s pelvic rehab group (administered by an experience physiotherapist) displayed statistically significant differences in physical function, pain, sexual worry, sexual activity, and sexual/vaginal function. Gynecological cancer and treatment procedures are potentially a fourfold assault: on sexual health, body image, sexual functioning, and fertility. Sexual morbidity is an undertreated problem in gynecological cancer survivorship that is known to occur early and to persist beyond the period of recovery (Reis et al 2010). We have a good and growing body of evidence that pelvic rehab, delivered by skilled therapists, has the potential to address each of these issues. And perhaps, most encouraging, here is Yang’s conclusion: ‘…‘Pelvic Floor Rehab is effective even in gynecological cancer survivors who need it most.’ (Yang 2012)
Interested in learning more about the role of pelvic rehab in gynecologic cancer survivorship? Join me in White Plains in August!
The following comes to us from Herman & Wallace faculty member Michelle Lyons. Michelle travels the world spreading the word about pelvic rehabilitation and the powerful benefits it can have on a patient's everyday life. Michelle will be teaching her newest course, "Oncology and the Female Pelvic Floor: Female Reproductive and Gynecologic Cancers" in White Plains, NY this August 14 - 15. Join her to learn more about evaluating and treating oncology patients.

According to the Scientific Network of Female Sexual Health and Cancer, ‘Sexuality is an experience that really is at the intersection of mind, body and relationship, and cancer treatment can impact all three of those elements”. Dr Sharon Bober of Dana Farber says ‘Part of the problem is that doctors are so focused on saving a cancer patient's life that they forget to discuss issues of sexual health. My sense is that it's not about physicians or health care providers not caring about your sexual health or thinking that it's unimportant, but that cancer is the emergency, and everything else seems to fall by the wayside".
If you harness the power of Google to look up female sexual dysfunction after gynaecologic cancer, you may see phrases like ‘Possible sexual side effects…’ or ‘Cancer treatment can cause physical changes that make having sex more difficult’ or even ‘cancer treatments may make intercourse painful’. To call these descriptions ‘understatements’ does not really do them justice.
For many women post-gynaecological cancer, resuming sexual function can be a multi-faceted problem. Issues can range from dealing with Cancer Related Fatigue and nausea, vomiting or diarrhea to physical changes in the size and shape of the vaginal canal. Cancer treatments can also cause hormone imbalances and tissue damage. Add to this issues with post-surgical/radiation adhesions, a disruption to the ability to produce lubrication, challenges to the musculo-skeletal systems within the hips and the pelvis as well as the onset of medically induced menopause….well you get the picture.
In a 2009 paper, ‘Interventions for sexuality after pelvic radiation therapy and gynaecological cancer’, Katz talks about the fact that ‘…very little attention has been paid to the sexual difficulties women experience after radiation to the sexual organs. There are a limited number of interventions for the woman who has been treated for gynaecological cancer with radiation. These focus on the provision of information and some specific suggestions related to treating vaginal dryness, the need for vaginal dilatation after radiation therapy, and management of fatigue. In ‘A systematic review of sexual concerns reported by gynaecological cancer survivors’ (Abbot Anderson 2012), the author points out that common concerns in the physical dimension were dyspareunia, changes in the vagina, and decreased sexual activity.
In the psychological dimension, common concerns were decreased libido, alterations in body image, and anxiety related to sexual performance. And in the social dimension, common concerns were difficulty maintaining previous sexual roles, emotional distancing from the partner, and perceived change in the partner's level of sexual interest.
The good news is that you can return to a normal sex life after surviving gynaecological cancer – particularly with the help of a skilled pelvic rehab provider.
In part 2 of this blog series, I will look at specific interventions in sexual rehab for the gynaecological cancer survivor. Interested in learning more about pelvic rehab and oncology? Join me in White Plains in August!
Pain associated with menstruation is known as dysmenorrhea, and more than half of women have pain related to their period for 1-2 days per month, according to The American College of Obstetricians and Gynecologists. Primary dysmenorrhea is related to menstruation, and often begins within a short period of time once menses occurs, whereas secondary dysmenorrhea is often related to a condition within the reproductive tract such as endometriosis or fibroids. In the medical office, a medical history, a pelvic exam, and possibly an ultrasound or laparoscopy will be completed. Treatment may include medications such as NSAIDs which target the prostaglandins that often lead to symptoms of dysmenorrhea, birth control pills, or surgeries.

A recent literature review asked if physiotherapy can help with symptoms of primary dysmenorrhea. Of the articles reviewed, 186 were chosen, and included a range of articles from descriptive, experimental studies to prospective, randomized controlled studies. A variety of interventions and approaches were included in the review, such as TENS, abdominal massage, acupuncture, cryotherapy and thermotherapy, connective tissue, Pilates, and belly dance. All of the approaches demonstrated some therapeutic benefit, either in response to the immediate application of the intervention, or up to a few months after the intervention was applied or instructed.
This literature review echoes a prior systematic review that evaluated the effectiveness and safety of acupressure, acupuncture, aspirin, behavioral interventions, oral contraceptives, and other supplements, procedures, and complementary and alternative medical interventions. Click here to view the full-text article. In that particular review, the authors reported the following:
- high-frequency TENS reduces pain (but less so than ibuprofen)
- acupressure may be as effective as ibuprofen
- topical heat may be as effective as ibuprofen and more effective than paracetamol
The bottom line from this research should be that we as pelvic rehabilitation providers need to help patients address pain and symptoms from dysmenorrhea. Clearly, there are many pathways to achieve symptom reduction, and some, such as TENS or topical heat, are easily carried out on an independent basis. How are you reaching adolescent girls who may develop primary dysmenorrhea? In clinical practice, talking with their parents, or reaching out at the community level to schools, churches, camps, gyms, or coaches may provide an opportunity to provide education and help. If you would like to learn more about myofascial release techniques for the abdomen and pelvis, check out the Myofascial Release for Pelvic Dysfunction continuing education course taking place next month in Illinois!
Today we hear from Herman & Wallace instructor Dustienne Miller CYT, PT, MS, WCS. Dustienne instructs the Yoga for Pelvic Pain course. Join her next month at Yoga for Pelvic Pain, Cleveland, OH on July 18 and 19!

We all know yoga can help chronic headaches, insomnia, anxiety, low back pain, and a myriad of other conditions. How can we apply the principles and benefits of yoga to the treatment of chronic pelvic pain?
Breathing
As rehab professionals who treat chronic pelvic pain, we know how critical it is for our clients to learn how to downtrain the nervous system. Breath awareness and training are a useful tool in reducing sympathetic nervous system override. Some clients may not have the awareness that they are holding their breath because of pain, or even anticipation of pain. Because of the direct mechanical relationship between the diaphragm and the pelvic floor, breath holding can lead to pelvic floor muscle holding. By building awareness, which is a learned skill, the client begins to notice and eventually control non-optimal breathing patterns.
Yoga offers several types of pranayama, or breathing techniques. Integrating breath with gentle movement has proven to be highly beneficial for men and women with chronic pelvic pain. Simple belly breathing lowers heart rate, blood pressure, and anxiety levels. For more detailed instructions on two pranayama, dirgha (3 part breath) and ujjayi (ocean-sounding breath), please click here.
Grounding
Grounding techniques decrease dissociation and anxiety. Two easy postures to practice in the clinic are Seated and Standing Mountain Pose (Tadasana). When practicing Seated Tadasana, encourage your patient to feel the ischial tuberosities heavy into the chair while imagining a string lifting up the spine and through the top of the head. When practicing Standing Tadasana, offer the imagery of a magnetic pull from the soles of the feet into the earth. For more detailed instruction on Tadasana, please click here.
Being Present
Negotiating medical system can leave clients with chronic pelvic pain feeling traumatized. Sadly, the percentage of men and women who have experienced additional traumas (ie: verbal abuse, sexual abuse) are quite high. Training the mind-body-spirit connection is helpful for the client to stay in the present moment rather than think about past painful experiences or anticipate future expectations of pain. Encourage the client to move at their pace and comfort level. Teach them gentle, loving acceptance of themselves and where they are in their healing journey. Clinicians must be mindful to avoid any potential trauma triggers (ie: teaching Supta Badha Konasana, butterfly/adductor stretch, in an open gym area). An excellent book to read to enhance your understanding of the delicacy of this subject is Overcoming Trauma through Yoga by Emerson and Hopper.
Calling all Pelvic Rehab tweeters! On June 24th, there will be a tweetchat hosted by 'Living Beyond Breast Cancer' to discuss and explore the effects of breast cancer on sexual health. Topics will include:
- How diagnosis and treatment side effects can affect intimacy and sexuality
- How to communicate with your cancer care team and partner
- Tips and suggestions for managing these side effects

Now, while I think it is brilliant that we are talking about sexuality during and after cancer, the panel has no input from pelvic rehab providers! We have so much to offer women in terms of sexual rehab in an oncology setting but if our colleagues and patients don't know about us.....
So some along and join the conversation on twitter on the 24th - don't forget to use the hashtag #LBBCchat. Hope to see you there to help raise the profile of pelvic rehab in the world of oncology.
Interested in learning more about sexual rehab after gynecologic cancer? Join me in White Plains NY this August!
Today we hear more from Susannah Haarmann, PT, WCS, CLT about how pelvic rehabilitation practitioners are suited to contribute to a breast oncology patient's medical team. Susannah will be sharing more insights and treatment tools at the Rehabilitation for the Breast Cancer Patient course taking place June 27-28 in Maywood, IL.

Most pelvic rehab practitioners are incredible problem solvers and independent thinkers. We understand that often our referrals from a physician occur after a battery of tests and ineffective medical interventions. We may agree to treat a patient only to find that the diagnosis is vague and the patient often feels lost and broken. So we take out our sleuth caps, ask as many subjective questions as it takes and see where our objective examination leads us. Afterwards we paint a picture of our findings, focus the patient on what is working, tell them where we are going to start and how we are going to build one brick at a time.
The same is true for rehabilitation and breast oncology. Most physicians don’t understand how our work as therapists can complement and alleviate the side effects of mainstream medical intervention, but when the pain medication no longer works, we are there. When the range of motion no longer exists to get the patient’s arm into a cradle for breast radiation, we are there. And when the patient walks in our door, we are there, quite often for a period of time that extends well beyond after treatments cease, because the potential side effects of breast cancer, if they occur, may take years or even decades to show up. The rehab practitioner understands how to prepare the patient, without fear, for what the road ahead may look like. The purpose of this education is to empower patients to serve as their own best advocates. Pelvic practitioners and breast oncology specialists are noted for their exceptional manual skills. We are also versed to pounding the pavement educating physicians, patients and other therapists alike about who we can serve and how we can be of service. We are definitely a unique breed of therapists.
The Rehabilitation for the Breast Cancer Patient course will add to the pelvic rehab practitioner's current knowledge allowing them to become a specialist. Consider the following:
A therapist understands the biomechanics of a shoulder joint and function, but do they understand how the effects of radiation, reconstruction procedures and impairments in the lymphatic system as a side effect of cancer treatment might prevent optimal upper extremity function?
A therapist may understand peripheral neuropathy and balance training or osteoporosis and aging, however, do they understand which chemotherapeutic and hormone therapies may cause these side effects and how the prognosis may differ depending upon which medical intervention was used?
A therapist may commonly treat back pain, but do they understand how a plan of care might be altered to accommodate for a patient who experienced a TRAM flap or latissimus dorsi reconstruction?
A therapist may be able to initiate a post-operative rotator cuff strengthening program for the upper extremity, but if the patient has a history of lymphedema, how do these parameters change?
A therapist may have advanced manual therapy skills, but how might one use these skills to identify and treat lymphatic cording or set safe parameters for working around radiated tissue to restore optimal function?
These are just a few of many examples of what constitutes a specialist in the field of breast oncology and each of these questions and more will be covered in detail in the course Rehabilitation for the Breast Cancer Patient.
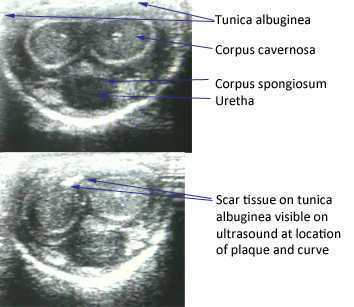
The American Urological Association issued new guidelines in May of this year for the diagnosis and treatment of Peyronie's. The disorder, which you can read more about at this link, often leads to a curvature in the penis that can be painful, or that can lead to impaired sexual or urinary function. While the exact mechanism leading to Peyronie's is still being researched, what is known is that plaques (sometimes calcified) may form in a deep layer of thick connective tissue called the tunica albuginea that surrounds the penis.
In the clinical guidelines, the authors state that a diagnostic process should include documentation of the signs and symptoms of Peyronie's disease. This can include a careful history (assessing any penile deformity, limitations in sexual function, penile pain, and level of distress). In the medical office, an intracavernosal injection (check here for a Medscape article describing an algorithm) can be completed. The authors also state, in line with expert opinion, that a provider should only evaluate a patient's Peyronie's disease when possessing "…the experience and diagnostic tools to appropriately evaluate, counsel, and treat the condition." In regards to pelvic rehabilitation, understanding the condition and encouraging the patient to visit a medical provider who is appropriately trained to manage Peyronie's is valuable. Establishing a baseline for the amount of dysfunction and curvature aids the patient and physician in determining current and future care planning.
Available treatments include education about possible treatments as well as adverse reactions to medical treatment. Interventions might include oral NSAIDs, intralesional injections (to reduce the amount of scar/thickened tissue or pain), and surgeries. Surgical options include procedures to remove the plaque or scar tissue, remodel the penile tissues after plaque removal, and for more severe cases, to implant a penile prosthesis. (Recommendations for treatments to avoid due to potential for harm or for lack of evidence are also listed in the article.)
The role of pelvic rehabilitation is emerging for men who present with genital pain, deformity, or pelvic dysfunction. There are certainly comorbid dysfunctions that we can address, such as pelvic muscle dysfunction, bowel and bladder issues if present, and we can provide a significant amount of education about pelvic health. Therapists are also teaching patients to perform connective tissue mobilization on the penile tissues, and some therapists are directing manual therapy, dry needling, and other modalities to the tissues. Rehabilitation lacks, at this time, compelling evidence to support direct treatment to the tissues, and hopefully that research will be seen in the near future. The authors of the new guidelines conclude that "…The most effective approach for a particular patient is best determined by the individual clinician and patient in the context of that patient’s history, values, and goals for treatment." This sounds to me like an effective approach for every patient who struggles with a condition that lacks a clear understanding of etiology and best treatments. These guidelines are a step forward in management of patients who deal with the frustrating condition, and the guidelines will be updated, according to the article, as the science advances.
If you would like to learn more about the rehabilitation implications of Peyronie's, and the potential and current roles of therapists in male pelvic health, you have two opportunities this year to attend the Male Pelvic Floor course , August in Denver, and November in Seattle. We expect the Seattle to course to sell out, and it's filling up fast, so check your calendar and come join us at the Male course.
Today we hear from Susannah Haarmann, the instructor for Rehabilitation for the Breast Cancer Patient. If you want to learn how to implement your pelvic rehab training with breast oncology patients, join Susannah in Maywood, IL on June 27th and 28th.

Effective pelvic rehab practitioners demonstrate many skills which are especially suitable to treat people with breast cancer, however, the first idea that comes to mind is that they understand what my friend refers to as, ‘the bikini principle.’ She remarked this week that I treat the ‘no no’ areas; the private places that we rarely share…with anyone. The reproductive regions of the pelvis and chest wall both consciously and subconsciously are associated with a plethora of personal psychological and social connotations. A pelvic health practitioner has a raised level of sensitivity to working with this patient population; there is no true protocol in this line of work, effective treatment will require a deeper level of listening and being present with the patient, and a person’s healing of the pelvic region is likely to go beyond the physiologic realm.
The biopsychosocial model of treatment is especially pertinent to the pelvic and breast oncology specialties. The breasts have great biological importance for sexual reproduction and nurturing offspring. Psychologically, breasts represent femininity for many women (and imagine how the story would change for a male with breast cancer.) Furthermore, different societies tend to create a host of rules and guidelines about what is ‘breast appropriate.’ The rehab practitioner understands that a person’s perceptions of their breasts are unlike any others and the same holds true for their cancer journey and goals with therapy.
The pelvic practitioner understands the importance of a straight face; if you have been in the field long enough something completely surprising is bound to occur, but in the day in the life of a pelvic rehab practitioner, no matter how shocking, we’ve seen it before, right? The breast oncology practitioner is going to visualize radiation burns that make their own chest wall hurt upon seeing it. Practitioners will encounter the most frustrating of severe functional deficits that could have been easily avoided had there been the opportunity for earlier intervention. The rehab practitioner providing breast oncologic care understands the story is complex, the road may be long, and although our role revolves around the body, the side effects of our treatment may have much greater reward beyond just physical function.

Today we are happy to celebrate Aline Flores, PT, PRPC! Aline is one of the newly minted Certified Pelvic Rehabilitation Practitioners, having passed the exam last month. Here's what she had to say about her career in pelvic rehab. Congratulations, Aline!
Tell us about your clinical practice
This year I opened Natura Physical Therapy, a small private practice specializing in pelvic pain and breast cancer rehabilitation. Manual therapy is a big part of our approach to patient care. I often utilize myofascial release, connective tissue manipulation, trigger point therapy, and manual lymphatic drainage during treat sessions and prescribe 2-3 specific exercises for patients to complete at home. I also provide education on the neurological/physiological/emotional response to pain and teach techniques for patients to be able to modulate this response, including breathing exercises and down training techniques. The majority of my patients are high stressed, overwhelmed and extremely hard on themselves. Helping patients become more compassionate towards themselves is a huge accomplishment.
How did you get involved in pelvic rehabilitation?
I was immediately interested in women’s health when I graduated from physical therapy school in 1997. I sought out a part time position to work/train with a therapist who was treating women with urinary incontinence. At that time I was only treating 1-2 pelvic patients a week primarily using biofeedback and muscle re-education. A year later I was hired by a hospital that was just starting a pelvic health program. Over the years I have been able to help this program grow from very basic pelvic health rehabilitation to treating much more complex pelvic health issues of like vulvodynia, pudendal neuralgia, and interstitial cystitis.
What/who inspired you to become involved in pelvic rehabilitation?
There have been so many women in pelvic rehabilitation that have inspired me and continue to inspire me. Elizabeth Nobel and Holly Herman were definitely early inspirations for me, as therapists in the founding of pelvic rehabilitation. I am always impressed the therapists who are currently making a huge impact with educating the medical community on the value of physical therapy in pelvic health issues. But, my biggest inspiration comes from my patients. Every day I learn something new from one of my patients. Whether it is a better understanding of their experience, or something that has worked, or doesn’t work for them, I am continually improving as a therapist by listening to my patients.
What patient population do you find most rewarding in treating and why?
I really enjoy working with patients with complex pelvic pain. These can be the most challenging patients to work with, but they are also the most rewarding. They keep me thinking critically. Usually these patients have a physical and an emotional component, but often have been told or assume that their symptoms are “all in their head”. It is very rewarding when I can explain the connection between the body, the nervous system and emotion, and the patient, finally feels understood. It is truly an honor to be able to work with these patients as they progress from a very difficult experience to a much more empowered state, where they have better understanding and control of their symptoms.
If you could get a message out to physical therapists about pelvic rehabilitation what would it be?
Pelvic physical therapy is much more than just “Kegels”. Issues involving bowel, bladder and sexual functioning are important activities of daily living that can have a significant musculoskeletal cause. Every physical therapist should have a basic understanding of pelvic floor muscle functioning, even if they don’t directly treat these conditions. The best pelvic rehabilitation therapists are good orthopedic therapists first.
What motivated you to earn PRPC?
Taking the PRPC exam was a challenge to myself to critically think about my knowledge base and how I practice. Although, I try to stay up to date on the most current research on a regular basis, preparing for the exam, encouraged me to be more though and consistent with my review.
What is in store for you in the future?
I hope to keep learning every day. I also plan being more involved in teaching physical therapists interested in pelvic health.
By accepting you will be accessing a service provided by a third-party external to https://www.hermanwallace.com/
All Upcoming Continuing Education Courses



Pelvic Function Level 1 - In-Person - Greensboro NC - June 7 - 8 2025 - SOLD OUT
Jun 7 2025 - Jun 8 2025

Nutrition Perspectives for the Pelvic Rehab Therapist - Remote Course - June 7 - 8 2025
Jun 7 2025 - Jun 8 2025





Pelvic Function Level 1 - Satellite - Torrance CA - June 14 - 15 2025 - SOLD OUT
Jun 14 2025 - Jun 15 2025

Pelvic Function Level 1 - Satellite - Long Beach CA - June 14 - 15 2025 - SOLD OUT
Jun 14 2025 - Jun 15 2025

Pelvic Function Level 1 - Satellite - Woodbury NY - June 14 - 15 2025 - SOLD OUT
Jun 14 2025 - Jun 15 2025


Pelvic Function Level 1 - Satellite - New York NY - June 14 - 15 2025 - SOLD OUT
Jun 14 2025 - Jun 15 2025

Pain Science for the Chronic Pelvic Pain Population - Remote Course - June 21 - 22 2025
Jun 21 2025 - Jun 22 2025

Dry Needling and Pelvic Health - In-Person - Atlanta GA - June 21 - 22 2025 - SOLD OUT
Jun 21 2025 - Jun 22 2025



Mobilization of Visceral Fascia - Gastrointestinal - Satellite Lab Course - St. Petersburg FL - June 27 - 29 2025
Jun 27 2025 - Jun 29 2025

Mobilization of Visceral Fascia - Gastrointestinal - Satellite Lab Course - Self-Hosted - Jun 27 - 29 2025
Jun 27 2025 - Jun 29 2025

Mobilization of Visceral Fascia - Gastrointestinal - Satellite Lab Course - Sellersville PA - June 27 - 29 2025
Jun 27 2025 - Jun 29 2025

Mobilization of Visceral Fascia - Gastrointestinal - Satellite Lab Course - Milwaukee WI - June 27 - 29 2025
Jun 27 2025 - Jun 29 2025

Mobilization of Visceral Fascia - Gastrointestinal - Satellite Lab Course - Medford OR - June 27 - 29 2025
Jun 27 2025 - Jun 29 2025

Mobilization of Visceral Fascia - Gastrointestinal - Satellite Lab Course - Bartlett IL - June 27 - 29 2025
Jun 27 2025 - Jun 29 2025

Mobilization of Visceral Fascia - Gastrointestinal - Satellite Lab Course - Cedar Knolls NJ - June 27 - 29 2025
Jun 27 2025 - Jun 29 2025

Mobilization of Visceral Fascia - Gastrointestinal - Satellite Lab Course - Marysville OH - June 27 - 29 2025
Jun 27 2025 - Jun 29 2025

Mobilization of Visceral Fascia - Gastrointestinal - Satellite Lab Course - New Orleans LA - June 27 - 29 2025
Jun 27 2025 - Jun 29 2025

Mobilization of Visceral Fascia - Gastrointestinal - Satellite Lab Course - Albany NY - June 27 - 29 2025
Jun 27 2025 - Jun 29 2025

Mobilization of Visceral Fascia - Gastrointestinal - Satellite Lab Cource - Amherst OH - June 27 - 29 2025
Jun 27 2025 - Jun 29 2025

Mobilization of Visceral Fascia - Gastrointestinal - Satellite Lab Cource - Paso Robles CA - June 27 - 29 2025
Jun 27 2025 - Jun 29 2025

Mobilization of Visceral Fascia - Gastrointestinal - Satellite Lab Course - Detroit MI - June 27 - 29 2025
Jun 27 2025 - Jun 29 2025



Pelvic Function Level 1 - Satellite - Tampa FL - June 28 - 29 2025 - SOLD OUT
Jun 28 2025 - Jun 29 2025


Pelvic Function Level 1 - Satellite - Waco TX - June 28 - 29 2025 - SOLD OUT
Jun 28 2025 - Jun 29 2025



Pelvic Function Level 1 - Satellite - Milwaukee WI - July 12 - 13 2025 - SOLD OUT
Jul 12 2025 - Jul 13 2025

Modalities and Pelvic Function - In-Person - Houston TX - July 12 - 13 2025
Jul 12 2025 - Jul 13 2025
Pelvic Function Level 1 - Satellite - Denver CO - July 12 - 13 2025 - SOLD OUT
Jul 12 2025 - Jul 13 2025

Pelvic Function Level 2B - Satellite - Sellersville PA - July 19 - 20 2025
Jul 19 2025 - Jul 20 2025