

Pilates has always had a place in rehab and was used frequently by those (think ballet dancers and performers) who needed a system of exercise that could challenge the neuromuscular system to bring them back to a high level of function. But Joseph Pilates created his “Method” to heal himself—he suffered from asthma, rickets, and rheumatic fever—and in doing so, made it suitable for all types of people at all stages of health and wellness.
Do you long to try that Reformer in your clinic but feel you have not had the training necessary to use it safely beyond a glorified squat machine? Come experience Pilates movement in my new course, Pilates Therapeutic Exercise in Pelvic Health, scheduled for May 3-4, 2025. By using your therapeutic exercise training, we will choose appropriate traditional Pilates exercises to apply to common pelvic floor and pelvic girdle dysfunction. This course is meant to focus on specific diagnoses like prolapse prevention, urinary incontinence, and postpartum abdominal wall activation. This is not Pilates training—there are many suitable courses for this goal - but rather it is to whet your appetite to further your training and give you explicit examples of Pilates exercises to help your patient.
We will review how to safely set up the reformer for patients and see how select exercises can transform core activation by doing rather than telling folks about the movement. Using the Reformer is a wonderful neuro reeducation tool -- utilizing springs, one can instantly create tension that will act as an active assist for muscle groups or modify it to be one that is resistive, creating activation of muscle contraction. Additionally, you can access many developmental postures on the Reformer that can help your patient succeed. Combined with good verbal and tactile cues, the Reformer is a go-to for my pelvic floor patients with pain, ROM issues, and/or weakness, and I can’t wait to share!
AUTHOR BIO
Pam Downey, PT, MSPT, DPT, WCS, BCB-PMD, PRPC
 Pam Downey, PT, MSPT, DPT, WCS, BCB-PMD, PRPC (she/her) is a Board Certified Clinical Specialist in Women’s Health Physical Therapy and Board Certified in Biofeedback for Pelvic Muscle Dysfunction. Owner of Partnership in Therapy, a private practice in Coral Gables, Florida, she treats pelvic floor dysfunction, related urogynecological and colorectal issues, spine dysfunction, osteoporosis, and complaints associated with pregnancy and the postpartum period. Her mission is to educate and integrate healthy lifestyles for patients on the road to wellness.
Pam Downey, PT, MSPT, DPT, WCS, BCB-PMD, PRPC (she/her) is a Board Certified Clinical Specialist in Women’s Health Physical Therapy and Board Certified in Biofeedback for Pelvic Muscle Dysfunction. Owner of Partnership in Therapy, a private practice in Coral Gables, Florida, she treats pelvic floor dysfunction, related urogynecological and colorectal issues, spine dysfunction, osteoporosis, and complaints associated with pregnancy and the postpartum period. Her mission is to educate and integrate healthy lifestyles for patients on the road to wellness.
Dr. Downey has been honored to teach with the Herman & Wallace Institute since 2006. She is an Adjunct Professor in the Physical Therapy Program at the University Of Miami Miller School of Medicine in Coral Gables, Florida, and Nova Southeastern University in Fort Lauderdale, Florida. A certified Polestar Pilates Educator, she utilizes Pilates and therapeutic exercise interventions specifically designed for patients with pre/post-natal, pelvic floor muscle, and other lumbo-pelvic pain-related dysfunctions.
Dr. Downey received her Bachelor of Arts from Sarah Lawrence College and her Master of Science and Doctorate in Physical Therapy from the University of Miami School of Medicine. She is actively involved in professional activities of the Section on Women’s Health of the American Physical Therapy Association, presently sitting as Coordinator of Research Submissions for annual meetings and as a manuscript reviewer for the Journal of Women’s Health. Dr. Downey has lectured nationally and internationally at professional conferences and is the author of multiple published research articles and a book chapter on chronic pelvic pain in the medical text, Women’s Health in Physical Therapy.


This week The Pelvic Rehab Report sat down with Kate Bailey, PT, DPT, MS, E-RYT 500, YACEP, Y4C, CPI to discuss her career as a physical therapist and upcoming course, Restorative Yoga for Physical Therapists, scheduled for September 11-12, 2021. Kate’s course combines live discussions and labs with pre-recorded lectures and practices that will be the basis for experiencing and integrating restorative yoga into physical therapy practice. Kate brings over 15 years of teaching movement experience to her physical therapy practice with specialties in Pilates and yoga with a focus on alignment and embodiment.
Who are you? Describe your clinical practice.
My name is Kate Bailey. I own a private practice in Seattle that focuses on pelvic health for all genders and ages. I work under a trauma-informed model where patient self-advocacy and embodiment are a priority. My dog, Elly, assists in my practice by providing a cute face and some calming doggy energy. My patients often joke that they come to see her just as much as to see me, which I think is great. In addition to being a physical therapist, I’ve been teaching Pilates for nearly 20 years and yoga for over 10. They are both big parts of my practice philosophy and my own personal movement practice
What books or articles have impacted you as a clinician?
I have a diverse library of Buddhist philosophy, emotional intelligence, trauma psychology, human behavior, breathwork/yoga, and sociology and, of course, a bunch of physical therapy pelvic floor books. I also love a children’s book on emotional regulation or inclusion, even for adults. One of my favorite finds is the Spot series that gives kiddos different ways to use their hands to help deal with different emotions. I’ve used it for adults who need physical self-soothing options. There are so many, and I find that it's the amalgamation of information that really impacts my practice the most.
How did you get involved in the pelvic rehabilitation field?
I have a deep interest in the human experience and how culture and dissociation create mass-disembodiment and how hands-on work can be profound in how we experience our body. Pelvic rehab allowed me the opportunity to work more closely with people on areas that bring up the most shame, disembodiment, and trauma, and therefore have some pretty amazing possibilities to make an impact not only in their lives but how they act in culture. In many ways, I see my work in pelvic rehab as a point of personal activism in creating a more embodied, empowered, and powerful culture.
What has your educational journey as a pelvic rehab therapist looked like?
I knew I wanted to go into pelvic health from my second year in PT school. I’ve always been at bit…well, let’s call it driven. I did an internship with great therapists in Austin and then only considered full-time pelvic floor positions once licensed. I took as many courses as I could handle in my first couple years of practice, which worked well for me, but understandably is not the right path for all those entering this field for a number of reasons. I went through the foundational series, and then into visceral work as well as continued my yoga and Pilates studies. I continued my education in trauma and emotional intelligence which is both a personal and professional practice. I found that a blend of online coursework and in-person kept me satisfied with my educational appetite.
What made you want to create your course, Restorative Yoga for Physical Therapists?
I was a yoga teacher long before I became a PT. When I found my way into the specialty of pelvic floor physical therapy, this particular part of my yoga teaching became incredibly useful for patients who had high anxiety, high stress, and difficulty with relaxation and/or meditation. This course was a way for me to share some of my knowledge of restorative yoga with the community of health care providers, where it could not only be used as a means of helping patients, but also as a means to start valuing rest as a primary component of wellbeing.
What need does your course fill in the field of pelvic rehabilitation?
Learning about yoga as a full practice and understanding that it has many components is very useful in deciding which component would be a good match for a pelvic health patient. Is it strengthening from an active practice? Is it meditation or pranayama (breath manipulation)? Or is it supported rest? This particular course focuses on the lesser-known aspects of the yoga platform: breath, restorative practice, and a bit of meditation. I have clients all the time struggle with meditation because their nervous systems aren’t ready for it. So we look at breathing and restorative yoga both as independent alternatives, but also as a way to get closer to meditation. Learning how to help people rest, the different postures, how to prop, and how to dose is an important component of this class. As a bonus, giving the clinicians another skill for their own rest practice can be useful when feeling tired, overwhelmed, or burned out. All this under a trauma-informed, neuro-regulation-focused model is a lovely way to deepen one’s physical therapy practice.
What demographic, would benefit from your course?
People who are stressed out or who work with people who are stressed out. In particular, clinicians who work with people who have pelvic pain or overactivity in their pelvic floors.
What patient population do you find most rewarding in treating and why?
I love working with female-identifying patients that struggle with sexual health or those who are hypermobile and trying to figure out movement that feels good. I love working with all genders generally and do so regularly. There’s nothing quite like helping a male-identifying patient find embodiment and understanding of their pelvis in a new way. I think for me, working to dismantle female normative structures for those identifying as female, particularly in the realm of sexual health feels inspiring to me because it combines physical, emotional, spiritual health with going against the cultural standards of how those identifying as women fit into society, and being able to sit with the trauma of all types that so many people face.
What do you find is the most useful resource for your practice?
A pelvic floor model is great. The most important part of my practice is a conversation about consent, not only for internal work but for everything I offer during visits and also for patients to understand that they can give or retract consent with any medical provider for just about any service. Emergency procedures are a smidge different, but I hope my patients walk away with the understanding that the medical community is here to serve their embodied experience. My newest favorite resource is a series of metal prints that depict the emotional intelligence grid used in the RULER syllabus. I have a magnet that patients can use to identify how they are feeling and help develop their language for emotional and then somatic or interoceptive knowledge.
What has been your favorite Herman & Wallace Course and why?
There was nothing quite like PF1. I don’t think I’ll ever forget it. The instructors were Stacey Futterman Tauriello and Susannah Haarmann. I was still in grad school prepping for my internship and ended up being the model for labs which falls squarely in line with my upbringing as a dancer who wanted to understand everything from the inside out. It was a challenging weekend on pretty much every level. I went through phases of dissociation and total connection. It made me realize that my decision to enter health care after having a career in movement was the right one.
What lesson have you learned from a course, instructor, colleague, or mentor that has stayed with you?
Meet the patient where they are at first and validate that they live in an incredibly intelligent body. I think sometimes it’s so exciting to see the potential that patients have because, as clinicians, we’ve seen the progress of others. In yoga, there is a practice of the beginner’s mind. It asks the student to sit with an empty cup of knowledge and experience each practice with the curiosity of someone just being introduced to yoga. I have knowledge that may be helpful to patients. Patients have so much knowledge of their own body from their life experiences, some of which are conscious and so much of which is subconscious. The fun part is seeing how my experience and their experience match (or don’t sometimes) to then assess how to craft the care plan.
If you could get a message out to other clinicians about pelvic rehab what would it be?
That it's so much more than pelvic rehab. We get to talk to people about things that aren’t talked about and normalize the human experience. Pelvic rehab gives safety to patients to experience their bodies in all the sensations that come from having a nervous system: from sadness to joy to relief to fear. It's all in there and when we learn about those sensations from pelvic rehab, my hope is that it can flood into other areas of life.
What is in store for you in the future as a clinician?
Refining, learning, and seeing what else comes. Hoping to publish a book of cartoon organs shortly. But most importantly to create a safe space for patients to feel cared for and supported in my corner of Seattle.
Kate Bailey (She/Her)
Pelvic Floor Physical Therapy
Yoga & Pilates

Since the passing of Title IX in 1972, which protects people from sex discrimination in education or activity programs receiving federal funding, the number of females participating in sports has greatly increased. The National Federation of State High School Associations states that in 2011 nearly 3.2 million girls are participating in high school sports.
Unfortunately, a consequence of this increased participation in sports is a higher prevalence in urinary incontinence (UI) and stress urinary incontinence (SUI) in female athletes. Borin et al looked at the ability of nulliparous female athletes to generate intracavity perineal pressure in comparison to nonathletic women. The study demonstrated that higher mean pressures were generated by nonathletic women in comparison to the athletic women group and that lower perineal pressures in the athletic women were also related to number of games per year and time spent on sport specific workouts and strength training workouts.
UI and SUI are underreported in the general population and also in the athletic population. As health care professionals it is important to screen for UI and SUI in our clients. Physical therapy interventions using pelvic floor muscle rehabilitation have shown to decrease the severity of UI and SUI (Rivalta et al, Hulme). Rivalta used internal methods to improve the function of the pelvic floor muscle. Hulme’s success was achieved through activation of the pelvic floor muscles’ extrinsic synergists.
 |
 |
Pilates is often used in physical therapy as a therapeutic tool to improve lumbar stability with studies showing increases in abdominal strength (Sekendiz), trunk extensor endurance (Sekendiz) and to improve posture (Kloubec). Pilates is often also used in pelvic floor muscle rehabilitation and can easily be modified for low level clients. For example the use of resistance can assist supporting the weight of the leg. Practical proof, while lying supine in neutral lumbar spine position, stretch an arm and a leg away from center, notice the difficulty to maintain neutral spine. Now hold a resistance strap, which is also attached to the foot, and notice how maintaining neutral lumbar spine is easier to maintain (pictured above).
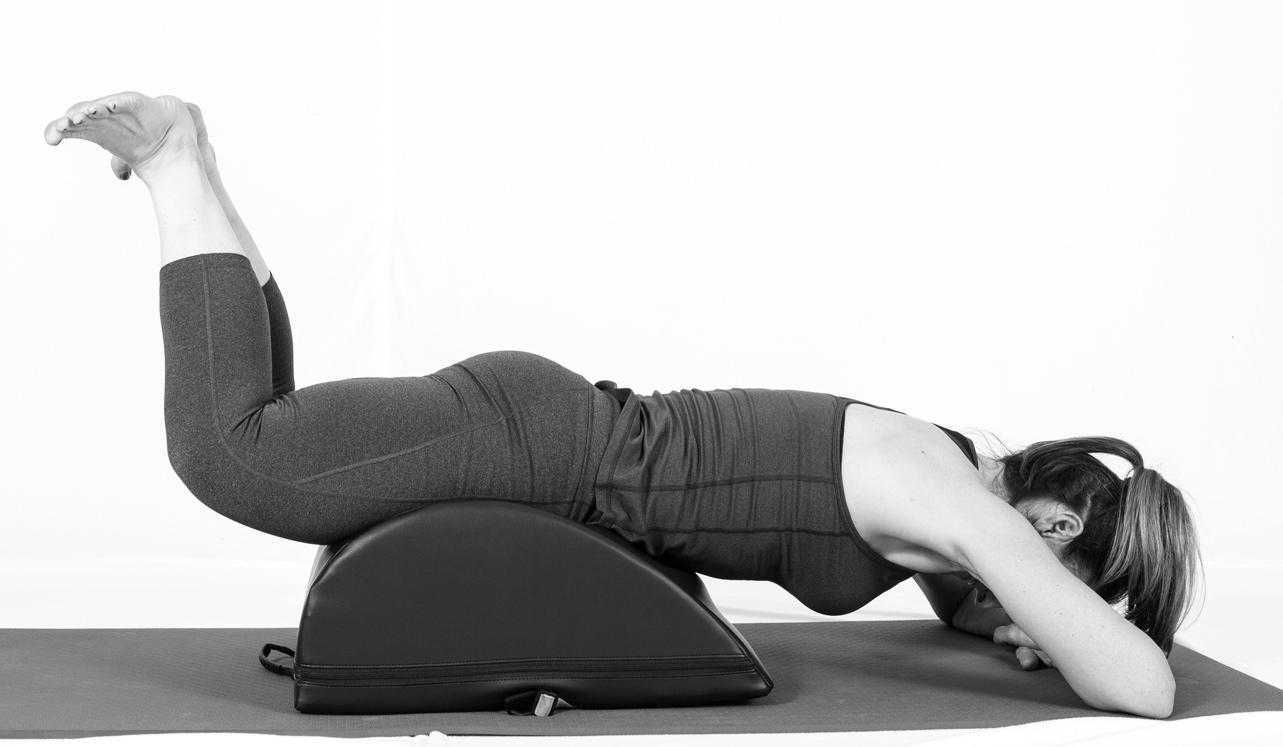
Pilates can also be modified for the higher level client or more athletic client. The use of arc barrels, BOSUs or the Hooked on Pilates MINIMAX (pictured belowy) allow the athletic client to achieve an inverted position, unloading the pelvic floor muscles. In the inverted position, pelvic floor muscles may be activated as intrinsic and/or extrinsic synergists of the pelvic floor muscles are also activated. These types of exercises may be more appealing to the athletic client ensuring continuation of the exercise post discharge from physical therapy.
 |
 |
Borin LC, Nunes FR, Guirro EC. Assessment of pelvic floor muscle pressure in female athletes. PMR. 2013; 5(3):189-193.
Hulme, Janet. Beyond Kegels 3rd edition, 2012 Phoenix Publishing Co. Missoula, Montana
Kloubec JA. Pilates for improvement of muscle endurance, flexibility, balance and posture. J Strength Cond Res. 2010;24:661-667.
Rivalta M, Sughunolfi MC, Micali S, De Stafani S, Torcasio F, Bianchi G, Urinary incontinence and sport. First and preliminary experience with a combined pelvic floor rehabilitation program in three female athletes. Health Care Women Int. 2010;31(5);330-334.
Sekendiz B, Altun O, Korkusuv F, Akin S, Effects of pilates exercise on trunk strength, endurance and flexibility in sedentary adult females. J Bodyw Mov Ther. 2005;9:52-57.

 Is there a consensus among physical therapists about the use and perceived effectiveness of Pilates exercise for low back pain? 30 Australian physiotherapists experienced with Pilates exercise were surveyed and asked about Pilates as an indication for low back pain. The results were published in Physical Therapy. Consensus at 100% was reached for benefits, indications, and precautions of Pilates exercise, and only 50-56% for risks and contraindications, respectively. Therapists agreed on indications such as maladaptive movement patterns, poor body awareness, poor flexibility, decreased lumbar spine mobility, poor breathing and postural control.
Is there a consensus among physical therapists about the use and perceived effectiveness of Pilates exercise for low back pain? 30 Australian physiotherapists experienced with Pilates exercise were surveyed and asked about Pilates as an indication for low back pain. The results were published in Physical Therapy. Consensus at 100% was reached for benefits, indications, and precautions of Pilates exercise, and only 50-56% for risks and contraindications, respectively. Therapists agreed on indications such as maladaptive movement patterns, poor body awareness, poor flexibility, decreased lumbar spine mobility, poor breathing and postural control.
The contraindications that were agreed on (but not as strong an agreement as the indications) included pre-eclampsia and unstable fractures. Agreement was reached that participation in Pilates exercise requires caution in the presence of unstable spondylolisthesis or significant lower extremity radiculopathy. The contraindications that were no agreed upon included cancer, severe osteoporosis, significant hypertension, and yellow psychosocial flags.
The physiotherapists did all agree that Pilates may help patients who have chronic low back pain by increasing function and confidence with movement, exercise, and activities, and additionally, that body awareness, postural control, and movement patterns may improve. Potential adverse events that may occur following Pilates exercise (and that were agreed upon) included aggravation of low back pain, or increased muscle tension. In relation to other potential risks of participating in Pilates exercise, inadequate training of instructors and inappropriate exercise prescription was listed. If you would like to learn more about Pilates exercise prescription for specific women’s health issues such as pelvic floor dysfunction, peripartum issues, and perimenopausal issues such as osteoporosis, check out the Institute’s new course on Pilates.

Today we hear from Martina Hauptmann, PT, PMA-CPI, instructor of "Pilates for the Pelvic Floor: Pelvic Floor Dysfunction, Osteoporosis and Peripartum". Join Martina this September 19-20 in Chicago, IL to learn how to incorporate Pilates into your treatment plans!
 Because the cost of staying in business is increasing and the insurance reimbursement rates are dropping, many physical therapy clinics are looking for cash based supplemental services (medically-orientated gym memberships, Pilates classes, yoga classes, durable exercise supplies etc). Offering Pilates as part of the physical therapy clinic’s therapeutic interventions will differentiate your clinic and may be marketed to physicians and the community to increase your clinic’s market share. Post rehabilitation, the offering of cash based Pilates wellness classes can increase the clinic’s bottom line, allowing for further rehabilitation of the client beyond the time frame allowed by insurances and improve retention of clients.
Because the cost of staying in business is increasing and the insurance reimbursement rates are dropping, many physical therapy clinics are looking for cash based supplemental services (medically-orientated gym memberships, Pilates classes, yoga classes, durable exercise supplies etc). Offering Pilates as part of the physical therapy clinic’s therapeutic interventions will differentiate your clinic and may be marketed to physicians and the community to increase your clinic’s market share. Post rehabilitation, the offering of cash based Pilates wellness classes can increase the clinic’s bottom line, allowing for further rehabilitation of the client beyond the time frame allowed by insurances and improve retention of clients.
Pilates is a system and philosophy of exercises based on the work of Joseph Pilates (1883-1967) that focuses on precision and optimal alignment. This approach requires the client to focus her mind on the exercise in order to increase motor control. Women are attracted to the Pilates method because of its gentle but effective nature. Offering Pilates as part of your therapeutic offerings is a great marketing tool to physicians and to the community as well as an effective method for instructing specific muscle re-training.
My course will focus on the application of the Pilates method to women’s health issues: incompetent pelvic floor, hyperactive pelvic floor, chronic pelvic floor pain, pre-natal, post-natal and osteoporosis with small props. The course will utilize equipment that you may have in the clinic already (physio balls, foam rollers, resistance bands, small balls BOSUs and introduction to the Hooked on Pilates MINIMAX and HANDIBANDs).
The course specifically will incorporate Pilates exercises that increase the function of the pelvic floor via the intrinsic and extrinsic synergists of the pelvic floor muscles. Rationale for modified Pilates exercises for clients that exhibit hyperactivity in the pelvic floor muscles (Carriere & Feldt, 2006), pre-natal (ACOG, 2002) and osteoporosis (Sinaki, 1984 and Sinaki, 2002) will be discussed and modified exercises performed. Finally discussion of post-natal issues of lumbo-pelvic pain and pubic symphysis pain will be incorporated and specific exercises for these issues performed (Richardson and Jull, 1995).
This course has a heavy emphasis on exercise. Participants in this course will be able to utilize all instructed exercises immediately following the course. I hope to see you there!
References:
Carriere & Feldt (2006). The Pelvic Floor. Stuttgart, Germany: Georg Thieme Verlag.
American College of Obstetricians and Gynecologists (2002).
Sinaki, Mikkelsen (1984). Post-menopausal spinal osteoporosis: Flexion versus extension exercises. Arch Phys Med Rehab. Vol 65, Oct, 593-596.
Sinaki et al. (2002). Stronger back muscles reduce the incidence of vertebral fractures: A prospective 10 year follow-up of postmenopausal women. Bone. 30(6); 836-841.
Richardson, Jull (1994). Muscle control-pain control. What exercises would you prescribe? Manual Therapy. 1, 2-10.

Today's post is written by faculty member Martina Hauptmann, who instructs the Pilates for Pelvic Dysfunction, Osteoporosis, and Peripartum course. Come learn how to apply Pilates in your practice this September 19-20 in Chicago, IL!
Treating the incompetent pelvic floor (urinary incontinence and pelvic organ prolapse) is a staple of therapists who have specialized in this complex area.
Ever since Dr. Arnold Kegel published his research “A Non-surgical Method of Increasing the Tone of the Sphincters and Their Supporting Structures” back in 1942 women have been strengthening their pelvic floor by conscious contraction of their perineum by either squeezing or lifting.
Another method to strengthen the pelvic floor is through the muscles that are extrinsic synergists to the pelvic floor musculature. The hip abductors, adductors, extensors and lateral rotators are extrinsically linked to the pelvic floor musculature. Except for one of the hip lateral rotators, the obturator internus, which by its anatomical attachments is actually an intrinsic synergist of the pelvic floor.
Pilates is an exercise method that seeks to increase a client’s strength, posture, control, and body awareness through precise exercises. The Heel Squeeze exercise is an excellent exercise to indirectly strengthen the pelvic floor via isometric contraction of the hip lateral rotators and hip extensors.
To perform the Heel Squeeze exercise, have the client lie prone with their legs hip distance apart, knees bent. The heels are touching and the toes pointing away from center. Draw the client’s awareness to their abdominals and have them slightly lift their stomach away from the mat. Instruct the client that she should continue with this contraction of her abdominals. Then as she exhales, the client squeezes her heels together and presses her pubic bone down into the mat. The client should hold this contraction for 5 seconds and do 8-12 repetitions.
All Upcoming Continuing Education Courses

Pelvic Function Level 1 - Satellite - Milwaukee WI - July 12 - 13 2025 - SOLD OUT
Jul 12 2025 - Jul 13 2025

Modalities and Pelvic Function - In-Person - Houston TX - July 12 - 13 2025
Jul 12 2025 - Jul 13 2025

Pelvic Function Level 1 - Satellite - Denver CO - July 12 - 13 2025 - SOLD OUT
Jul 12 2025 - Jul 13 2025




Pelvic Function Level 1 - Satellite - Des Moines IA - July 26 - 27 2025 - SOLD OUT
Jul 26 2025 - Jul 27 2025

Pelvic Function Level 1 - Satellite - Minneapolis MN - July 26 - 27 2025 - SOLD OUT
Jul 26 2025 - Jul 27 2025

Pelvic Function Level 1 - Satellite - Paso Robles CA - July 26 - 27 2025 - SOLD OUT
Jul 26 2025 - Jul 27 2025

Pelvic Function Level 1 - Satellite - St. Augustine FL - July 26 - 27 2025
Jul 26 2025 - Jul 27 2025

Pelvic Function Level 1 - Satellite - Virginia Beach VA - July 26 - 27 2025 - SOLD OUT
Jul 26 2025 - Jul 27 2025


Pelvic Function Level 1 - In-Person - Chicago IL - August 2 - 3 2025 - SOLD OUT
Aug 2 2025 - Aug 3 2025



Menopause Transitions and Pelvic Rehab - Remote Course - August 9 - 10 2025
Aug 9 2025 - Aug 10 2025









Pelvic Function Level 2C - Satellite - Palm Beach FL - August 16 - 17 2025
Aug 16 2025 - Aug 17 2025

Pelvic Function Level 2C - Satellite - New Orleans LA - August 16 - 17 2025
Aug 16 2025 - Aug 17 2025
Pelvic Function Level 2C - Satellite - Paso Robles CA - August 16 - 17 2025
Aug 16 2025 - Aug 17 2025


Pediatrics Level 1 - Treatment of Bowel and Bladder Disorders - Remote Course - August 23 - 24 2025
Aug 23 2025 - Aug 24 2025

Pelvic Function Level 1 - Satellite - Jacksonville FL - August 23 - 24 2025
Aug 23 2025 - Aug 24 2025

Pelvic Function Level 1 - Satellite - Chicago IL - August 23 - 24 2025 - SOLD OUT
Aug 23 2025 - Aug 24 2025


Rehabilitative Ultrasound Imaging Pelvic Health Satellite Lab Course - Self-Hosted - September 5 - 7 2025
Sep 5 2025 - Sep 7 2025
Rehabilitative Ultrasound: Orthopedic Topics Satellite Lab Course - Self-Hosted - September 5 - 6 2025
Sep 5 2025 - Sep 6 2025

Rehabilitative Ultrasound Imaging Pelvic Health Satellite Lab Course - Indianapolis IN - September 5 - 7 2025
Sep 5 2025 - Sep 7 2025
Rehabilitative Ultrasound: Orthopedic Topics Satellite Lab Course - Indianapolis IN - September 5 - 6 2025
Sep 5 2025 - Sep 6 2025
