Pelvic Rehab Report
The official Herman & Wallace blog. New blogs post every Friday on topics relating to the field of pelvic floor dysfunction.

Eating Disorders Awareness Week (EDAW), is February 26-March 3, 2024! It is an annual campaign to promote education about eating disorders. This week is also intended to provide hope and support for individuals and families affected by eating disorders. Awareness is key for both the public and the healthcare community.
We, as pelvic health providers, have the privilege to work with people of all genders with complex and often complicated medical histories. What are we really missing? What do we read (or not read) between the lines? What are cries for help that we are not hearing or noticing? As pelvic providers, we just need to keep our eyes, ears, and hearts open to our patients. The art of listening, observing and respectfully inquiring may be our greatest superpower. Imagine we are doing a puzzle without the puzzle box. Often it will take us time to gather the pieces and start to see the fuller picture. As health care providers, we carefully look at the whole puzzle - not just one piece… and sometimes this does take time.
Let’s take a look at a typical day in our busy clinical lives. Maybe you can relate. On our first visit with our patient, we are working hard (and sometimes fast) to try to get a thorough history, have appropriate functional outcome measures completed, ensure that all of the necessary “paperwork” is completed for our office or health care system, do our objective examination, pelvic muscle assessment, establish a prognosis, goals, a plan of care, etc. Does this sound familiar? How much can we fit into the time we are allotted at our workplace to get a picture of our patient? During this first visit do we get all of our answers? Or do we instead have a lot more questions?
We all see people struggling with eating disorders or people who have been recovering from an eating disorder - whether we are aware of this or not. The important thing to remember is that we do not treat eating disorders - we treat the individual who walks into our office with pelvic pain, constipation, abdominal pain, abdominal bloating, fecal incontinence, pelvic organ prolapse, urinary urgency, urinary incontinence, etc. We can ask some questions, do some observation, and have some conversations with our patients.
Many people have disordered eating patterns - perhaps eating too much or too little, following fad diets, having ideals of what they want their body should look like, etc. However, for some, their life may take a path that they did not expect from a multitude of biological, psychological, and social factors. Some of these factors include genetics/ family history, environment, societal / health care weight stigmas, trauma, sexual abuse, personality traits, brain chemistry, negative energy balance, hormonal levels, social support (or lack of), family dynamics and comorbid medical and/or mental health conditions (to name a few).
Eating disorders are mental illnesses with serious and sometimes fatal medical complications. Please understand - this illness is not about the food. Just eating “more” or “less” is not going to “cure” the illness. It is not that easy. What triggers an eating disorder may not be what keeps someone in the grips of it. Living with an eating disorder is distressing, consuming, life-sucking, isolating, secretive and painful. Having an eating disorder is NOT a choice. Treatment for eating disorders requires a team of support including mental health professionals, dieticians, primary care practitioners and specialists skilled with working with these individuals. We can be a part of this team. These disorders cause GI distress and nutritional rehabilitation for those who have to bring more nutrition into their body also causes GI distress. Recovering from an eating disorder is a complicated and often bumpy journey and we have the skills to help these people!

Here is a secret about eating disorders - they often ARE secrets. This is not something that someone may openly offer or even know for sure themselves. People with eating disorders are in all body sizes, genders, races and ages. We cannot make assumptions based on a person's weight or body size. Truthfully, people with atypical anorexia nervosa are often in bodies that would not trigger a clinical “alarm”, however, these individuals suffer from the same medical issues and complications as people with “typical” anorexia nervosa. Individuals in larger bodies may be utilizing purging behaviors such as vomiting, laxative use, may be binging and/or restricting food intake the same as someone in a smaller body. We cannot expect just a young, white, thin woman to have an eating disorder. They certainly may - but so may the person you just saw the hour before who is a thirty-year-old transgender woman, the 18-year-old male wrestler from the day before, the mother who is 2 months postpartum who is coming in this afternoon, or the 74-year-old woman you saw two hours ago.
We may see a person who avoids a mirror or is constantly checking their appearance. We may notice a person who is always cold and wearing layers. We may have someone who when we ask them about their relationship with food, clearly avoids the topic or tells us that they eat “ultra clean” and have limited many types of food groups in their “diet”. We may hear someone tell us many times how they do not want to gain weight so they will not consider eating more frequently, despite their painful constipation, because they “fast” for 22 out of 24 hours a day. They may also be able to give us calculated accounts of how much or how little they ate. Or, maybe they will tell us that they are so ashamed that they eat so much when they are stressed and how they cannot help it. Possibly, we may hear our patients tell us that they exercise every day, despite the weather, and sometimes more than once a day. Maybe they tell us that they haven’t been hanging out with their friends anymore and that no one understands them.
If you do notice that there are concerns, talk to your patient, let them know why you are concerned, and offer to help them find resources to provide support for them. If you do suspect someone is struggling with an eating disorder, provide them resources if they are agreeable. National Eating Disorders Association (NEDA), National Association for Anorexia Nervosa and Associated Disorders (ANAD), Eating Disorder Hope, National Alliance on Mental Illness (NAMI), Eating Recovery Center (ERC) are just a few of the great places to start.
Try to build a network of dieticians, mental wellness providers, primary care providers, GI specialists, and other practitioners who have interest, knowledge and expertise with people with eating disorders. This will likely not be easy to find. We have the skills to help these individuals during distress with active disorders and during recovery.
Join us in Eating Disorders and Pelvic Health Rehabilitation on April 6 and 7 to discover more about eating disorders and ways that we, as pelvic health professionals, can provide assistance and relief to these individuals as they struggle and as they recover. Learn more about the dangerous medical complications with eating disorders, how to identify individuals who may need support, and treatment options to assist these individuals on their journey to improved health. Explore ways to grow your clinical practice with this patient population. Looking forward to seeing you there!

In my first year of PT school, in the jumble of summer anatomy class and lab, the pelvic floor was briefly mentioned. The gist of the lesson was that it was a very in-demand field, there were not enough people doing it, and the majority of people affected were female. I was immediately intrigued, but also a little confused by the quick overview that was barely ever mentioned again until our special topics course 2 years later. By then, I was certain I wanted to learn more.
In my third year of PT school, I took the Herman & Wallace Pelvic Floor Level 1 (now Pelvic Function Level 1) course and entered my last clinical internship at a fully dedicated pelvic floor practice. The experience gave me exposure to the wide variety of pelvic floor issues that physical therapy can address. In school, it was mainly presented as something that was primarily addressed post-partum. In the clinic, it actually showed up as that coupled with a bulk of nulliparous patients of all genders and lifestyles with pelvic pain, complex cases with multiple co-morbidities, and incontinence in all age groups. This larger view of the field solidified my belief that pelvic floor rehab was being underutilized.
Through the following years, I worked in many different settings including hospital-based outpatient and private practices. Exposure to multiple populations across three states again broadened my view of pelvic rehab to something that could benefit so many people throughout their lifespan. In the summer of 2020, I began working under the mentorship of Raquel Perlis in her clinic in Wellesley, MA. Being one of the first pelvic rehab practitioners in the PT world, Raquel is widely known for her treatment of the chronic pelvic pain population. Together we addressed many cases of vaginismus, vulvodynia, SI joint pain, coccydynia, endometriosis, rectal pain, etc. Working with the pelvic pain population was both challenging and rewarding, as working with many chronic conditions in PT can be.
The experience of working with so many people suffering not just from the initial physical condition, but also from neglect, medical gaslighting, and shame, led to my decision to sign up for the Pelvic Rehab Practitioner Certification exam towards the end of my time in the Boston area in 2023. I knew I wanted to try to go out on my own in my next location and I believed that having the PRPC would give both me and my patients confidence in my skills as a practitioner operating independently for the first time. I had done most of my pelvic floor education with Herman & Wallace and mentors and for this reason, this was the best choice for me.
For me, seeing patients with pelvic pain has become my main interest. In my years of experience, no matter where in the country I am working, I see that the dismissal of pain, especially in women, LQBTQIA+, and nonbinary individuals, is all too common and often compounds the distress of those already suffering from physical discomfort. There have been multiple times when I or a colleague would be the first to acknowledge that a patient’s pain was even real. Too many were initially told by healthcare providers that the pain was in their heads or stemmed from anxiety. Of course, anxiety is often seen in the chronic pain population, but as a result of the pain they are experiencing, not the cause of it.
Gaslighting individuals with symptoms that are not easily explained has been an ongoing theme in the history of medicine and it continues to be an issue despite the advances we have made. It is estimated that innovation in the area of women’s health is at least 20 years behind other fields. We should not be dismissing what we do not know. The current structure of our healthcare system often does not give healthcare providers enough time or bandwidth to address complex pain and acknowledge what they cannot explain. That is the gap rehab providers like me seek to fill.
For me, patient education is without a doubt the most important aspect of my interaction with patients. Education is key to reducing anxiety over the unknown and giving people back power over their bodies. It is also preventative medicine. When a patient is taught how and encouraged to care for themselves, we prevent the recurrence of a condition or disease. Unfortunately, working together with patients to teach them how to care for themselves and repair their bodies is the important work that is often the first thing to be thrown out in a system built for acquiring as many high-paying codes in as little time as possible. Luckily, PTs and other rehab professionals are given a little more time with patients to help them understand their physical bodies and conditions.
Currently, I own and operate my own mobile pelvic PT clinic in Burlington, Vermont where I go to meet people where they are. This concept evolved over years of seeing busy individuals with long work hours, non-existent childcare, transportation issues, or all of the above struggle to make their recurrent follow-up PT appointments that often are scheduled for the middle of the day. My caseload now includes individuals as young as 15 as well as those who are middle-aged, post-partum, just out of college, and older adults.
Recently, I have been pursuing continuing education and training in helping people overcome pain and recover function post-op gender-affirming surgery, cancer treatment, and oncological surgery. I also have begun filling in as a teaching assistant at Herman & Wallace courses when I can. Education is not only important for patients, but I think it is also key to being an evolving practitioner and keeping the work ever new, interesting, and exciting. I hope to continue growing as an educator and eventually move into more teaching roles in the future.
BIO:
Rachel Martone, PT, DPT, PRPC, CYT graduated with her Doctorate of Physical Therapy from Hunter College in 2016 and has been working as a physical therapist in pelvic rehab for the past 8 years. Dr. Martone is a Certified Pelvic Rehab Practitioner with Herman & Wallace and has received her yoga teacher certification from Down Under Yoga. Currently, Rachel owns and operates her own mobile pelvic rehab clinic in Burlington, VT.
Rachel Kilgore, DPT, OCS, COMT, PRPC, PPCES graduated from Central Washington University with a Bachelor of Science (BS) in exercise science and a minor in nutrition in 2004 and completed her Doctor of Physical Therapy (DPT) at the University of Washington in 2007. Rachel practices in Seattle at Flow Rehab in the Freemont Neighborhood with Holly Tanner and focuses her patient care on orthopedics, female athletes, and women’s health conditions for bladder & bowel dysfunctions, pelvic, pain, pregnancy, and post-partum issues.
I have always been very particular about the precision of words. I have been known to ruminate about the origin, evolution, and application of words. As my husband always kindly says, I am an overthinker. This leads me to our nomenclature analysis for today, Diastasis.
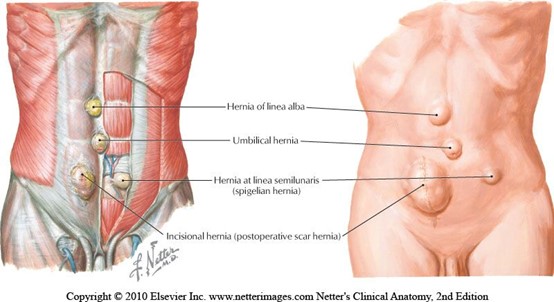 When teaching pregnancy and post-partum courses we always have healthy discussions about Diastasis Rectus Abdominus (DRA) as this is an important topic in the peripartum world. One question that always comes up is what is the difference between a hernia and DRA? If DRA is not a condition you deal with often in the clinic, it can be a bit confusing. According to the Merriam-Webster Dictionary diastasis means “an abnormal separation of parts normally joined together,” so DRA is often defined as a separation of the Rectus Abdominus muscles. I think the word separation is what causes the confusion. This word may lead some people to think there is an actual disruption of the abdominal tissue which is not the case. The rectus abdominus halves remain joined together by the linea alba. The linea alba is the tendinous raphe formed by interdigitating fascia of external/internal obliques and Transversus Abdominis. A DRA is an increase in the distance between the right and left Rectus Abdominus halves. If you stretch connective tissues (increase the distance between two ends), they may become thinner, lengthened, or weakened. A DRA is an increased distance between the right and left Rectus Abdominus halves that may result in lengthened, thinner, weaker tissue. In contrast, a hernia is an actual defect in the connective tissue. DRA and hernias are not the same thing; however, they can exist together.
When teaching pregnancy and post-partum courses we always have healthy discussions about Diastasis Rectus Abdominus (DRA) as this is an important topic in the peripartum world. One question that always comes up is what is the difference between a hernia and DRA? If DRA is not a condition you deal with often in the clinic, it can be a bit confusing. According to the Merriam-Webster Dictionary diastasis means “an abnormal separation of parts normally joined together,” so DRA is often defined as a separation of the Rectus Abdominus muscles. I think the word separation is what causes the confusion. This word may lead some people to think there is an actual disruption of the abdominal tissue which is not the case. The rectus abdominus halves remain joined together by the linea alba. The linea alba is the tendinous raphe formed by interdigitating fascia of external/internal obliques and Transversus Abdominis. A DRA is an increase in the distance between the right and left Rectus Abdominus halves. If you stretch connective tissues (increase the distance between two ends), they may become thinner, lengthened, or weakened. A DRA is an increased distance between the right and left Rectus Abdominus halves that may result in lengthened, thinner, weaker tissue. In contrast, a hernia is an actual defect in the connective tissue. DRA and hernias are not the same thing; however, they can exist together.
Let’s contrast these two conditions. Hernias can occur anywhere in the abdominal wall, whereas DRA is only at the midline. Hernia can strangulate intestines, but DRA does not as there is no hole or defect in the connective tissues. The only way to truly diagnose a hernia is by ultrasound. The only definitive treatment of a hernia involves surgery with closure of the hole, sometimes supported by mesh. Patients may elect to not have surgery if the hernia is small, is not painful, or if other conditions make surgery too risky. For diastasis, treatment rarely involves surgery. Hernias are disrupted fascia. Diastasis is lengthened, thinning, or weakened fascia.
 Diastasis Rectus Abdominus occurs commonly towards the end of pregnancy, with 66-100% of women having DRA by the end of the third trimester (Boissonnault & Blaschak, 1988; Mota et al, 2015). Mota et al. 2018 measured the distance between the two rectus halves in 84 primiparous women in the third trimester 2 cm below the umbilicus and found the average to be 49-79 mm. In contrast, a study of 150 nulliparous women (Beer et al.) showed the inter recti distance at that same point (2 cm below umbilicus) to be 16mm. However, DRA is not exclusive to the pregnant or postpartum person, they can exist in children and men as well.
Diastasis Rectus Abdominus occurs commonly towards the end of pregnancy, with 66-100% of women having DRA by the end of the third trimester (Boissonnault & Blaschak, 1988; Mota et al, 2015). Mota et al. 2018 measured the distance between the two rectus halves in 84 primiparous women in the third trimester 2 cm below the umbilicus and found the average to be 49-79 mm. In contrast, a study of 150 nulliparous women (Beer et al.) showed the inter recti distance at that same point (2 cm below umbilicus) to be 16mm. However, DRA is not exclusive to the pregnant or postpartum person, they can exist in children and men as well.
Another example of the word diastasis, where separation does not mean disruption, is with pubic symphysis diastasis. The words may be confusing. When a patient hears the word diastasis and is told it means separation, they may conclude they have a disrupted pubic joint. I think the definition of it from Stolarczyk et al. is much more descriptive and less likely to cause angst in a patient. “A pubic symphysis diastasis (PSD, diastasis symphysis pubis) is defined as excessive widening of the system of anatomical structures that make up the pubic symphysis (above the physiological norm of 10 mm), occurring during pregnancy or postpartum.”
This is another instance where the word separation may imply disruption when it just means increased distance.
Let’s return our thoughts to the title of this blog. I hope we are thinking about how the words we choose make our patients feel. Many of our patients receive a diagnosis and turn to the internet, where they may find confusing and even scary descriptions of their condition. If you were told that your abdominals had separated, doesn’t that sound scary? Would you feel nervous that your organs may fall out from your separated abdominals? I would have so many questions and fears! How will they get back together, what activities should I refrain from, can I even move? Wouldn’t the term separated make you feel scared to do anything? Think about the term separated shoulder, we hear it all the time in sports, we know it is a torn AC joint. There is an actual disruption of tissue, but DRA is not. As health care providers it is important that we use safe and encouraging words with our patients. Our role should be to educate them on their condition and make sure they understand the anatomy, physiology, and functional implications. We need to empower. The more a patient knows about their condition, the better choices they make regarding activity and lifestyle. Words are powerful.
References:
- Boissonnault, J. S., & Blaschak, M. J. (1988). Incidence of diastasis recti abdominis during the childbearing year. Physical Therapy, 68(7), 1082-1086.
- Mota, P., Pascoal, A. G., Carita, A. I., & Bø, K. (2018). Normal width of the inter-recti distance in pregnant and postpartum primiparous women. Musculoskeletal Science and Practice, 35, 34-37.
- Beer, G. M., Schuster, A., Seifert, B., Manestar, M., Mihic‐Probst, D., & Weber, S. A. (2009). The normal width of the linea alba in nulliparous women. Clinical anatomy, 22(6), 706-711.
- Stolarczyk, A., Stępiński, P., Sasinowski, Ł., Czarnocki, T., Dębiński, M., & Maciąg, B. (2021). Peripartum Pubic Symphysis Diastasis—Practical Guidelines. Journal of clinical medicine, 10(11), 2443.
Rivki Chudnoff, MSPT is instructing her course,Sex and Religion: Treating Conservative Religious Patients on March 10, 2024. At her private practice Hamakom Physical Therapy in Bogota, NJ she focuses on women’s health and pelvic health rehabilitation for women and children where she uses a biopsychosocial approach to guide her patients through the many challenges that they encounter along their journey to healing. Rivki has written extensively on women’s health issues and has presented on pelvic health internationally to sex educators, at community events, and at marriage retreats.
We were taught growing up that it was not polite to discuss sex, politics, or religion in the workplace…and then we became pelvic health providers.
Well, there goes sex.
If we are doing it right, and taking a thorough patient intake, we have mastered our sexual interviewing skills. We know how to ask (when appropriate) about sexual function as it pertains to our patient’s pelvic health.
But what about religion? What about when our patient’s cultural and religious backgrounds are important parts of the self they bring into our treatment rooms? It may be shaping their approach to healthcare, sexual function, and perhaps their relationship and views of their own bodies and our treatment.
And, what about us?
What about the clinical self we bring into the treatment room? We are not quite AI just yet. We each come from unique backgrounds, beliefs, origin stories, and values of our own. How can we bring our best, most professional selves into the treatment room when addressing patients with backgrounds and beliefs that may be different from our own or what is familiar to us?
Where does that leave us as healthcare providers as we try to engage our patients in a way that is both culturally sensitive and clinically effective?
That’s a whole lot to figure out on our own even with our PT and OT degrees. Like, what’s the range of motion? Can someone please get me a goniometer?
Sex and Religion: Treating Conservative Religious Patients was developed to help pelvic health providers navigate these questions and challenges that are often unique to our profession.
While there are so many religions and cultures, each with a myriad of their own customs and ideologies, this course provides the basics of Christianity, Hinduism, Islam, and Judaism as they pertain to sex and religious customs. Expert interviews included in this course provide an insider’s view into various religions' sexual attitudes and practices. We will explore some of the challenges that may face patients who come from conservative religious communities as they interface with the wild world of pelvic health. Participants will leave this course with practical skills for patient interviewing, treatment strategies, and creating a safe and comfortable space for both patients and providers.
It is my hope that this course will help both the seasoned and newer therapists open their skill sets to reach more diverse patient populations in their area.
But as for politics… I got nothing.

Can you tell me a little bit about who you are and your journey to pelvic rehab?
I graduated from Physical Therapy school year 2002 with a bachelor’s degree in physical therapy and finished my transitional doctorate here in the United States. Never did I imagine that I would find my path one day to treating pelvic floor disorders. My experiences were combinations of orthopedic rehabilitation, and pain management with in-patient and out-patient settings. I started practicing in the Philippines, went to the Middle East, and finally found my way to Illinois in 2011.
I am fascinated with how postural alignment and the coordination of the full body can affect one region of the body from distally to proximal, to centrally and peripherally. How a single whip of one body part - how the coordination of breathing and moving, stabilization of core/spine/pelvic floor/scapula can affect even your distal body region.
I love finding the cause of the problem in my patient and not only treating the main complaint. I want to understand what caused the issue. I feel accomplished when I can make my patients understand why they have the problems and symptoms they have and teach them to manage it. That’s when I feel the most accomplished with what my role in their life is.
I had been practicing as a pelvic floor therapist for more than 5 years before I finally decided to get my PRPC certification. Herman & Wallace has been my mentor from the moment I started my journey in this specialty. I learned a lot from Herman & Wallace and the continued learning fueled my passion for learning even more. Every time I learn a technique from assessment to holding and releasing tissues, and understanding facial connections, etc. I get more excited and involved. Every time I have a patient in front of me who tells me their story and issues, I just feel so blessed to be able to understand their problem and so thankful that I can touch their lives and help them get better. Thank you to all the dedicated Herman & Wallace instructors and facilitators!
What does a "day in the life" look like for you?
10 years ago, I was not as productive as I am now. Yes, I worked a lot, but my patient load was not near what it is now that I am a pelvic floor therapist. I worked as a full-time therapist at Jacksonville Memorial Hospital. I’m one of only 2 pelvic floor therapists and the only one treating male pelvic floor issues. On top of that, I also work part-time in my own clinic that I opened to serve patients in my area and others nearby who don’t have access to pelvic floor therapists. I have patients driving from 2 hours away because they cannot find a pelvic floor therapist. The waiting time for a new patient evaluation in the hospital where I work is 2-4 months. This is the main reason why I decided to open my own clinic, Netherine’s Physical Therapy, Pelvic Floor and Wellness. There is such a big need for pelvic floor therapists in our area. This is what God intended for me to do, and I’m loving the work.
What does your usual day look like?
My usual day is nonstop! A minimum of 24 units to 32 units in a day. One patient directly to another. Rushing through my one-hour lunch to have 30 minutes to call my own and then prepare again for my 1 pm patient. My caseload is 80% pelvic floor and 20% patients referred to me by colleagues (that are not improving after long-term treatment). As a pelvic floor therapist, I understand the relationship of the body from head to foot and from superficial to internal so I can easily create a POC that is more effective than when I was a basic orthopedic therapist.
I just love being a pelvic floor therapist. The music to my ears and heart is when my patient says- I’m not leaking anymore. I’m saving money because I don’t have to use pads or Depends. I have a bowel movement every day. I do not strain. I have a normal sex life. I don’t have anything falling “down there.” I feel more rested and more energized because I’m sleeping better at night. Thank you for not giving up on me.

Mora Pluchino, PT, DPT, PRPC is a Stockton University graduate with a BS in Biology (2007), and a Doctorate in Physical Therapy (2009). Mora's toolkit involves experience in a variety of areas and settings, including working with children and adults, including orthopedics, bracing, neuromuscular issues, vestibular issues, robotics training, and in 2016 she began treating Pelvic Health patients. Mora is active with Herman & Wallace as a Lead TA, faculty, member of the content team, and has written and instructs 3 of her own courses with HW including Pediatric Pelvic Floor Play Skills which is intervention-focused, and does not delve into specific pediatric diagnoses.
“I’m an expert at children’s behavior” said no experienced therapist (or parent or teacher) EVER. Working with kids is one of the most gratifying and frustrating, not to mention mystifying experiences I have ever had. What works for one child sends another into a temper tantrum. What one kid thinks is fun has another whining about how they may die of boredom. Ask the pelvic organ stuffies in my treatment what I’m talking about, they could tell you some stories!
Herman & Wallace has two amazing pediatric courses by Dawn Sandalcidi (Dawn Sandalcidi’s course Pediatric Incontinence and Pelvic Floor Dysfunction) that give such a great foundation to diving intro treating pediatric clients. I’ve taken them both myself and would not have been the clinician, teaching assistant or instructor I am without them. In these classes you can learn all of the diagnoses, latest research and treatment protocols from someone who has been a leader in pediatric pelvic floor therapy for years.
Why then did I feel the need to write a course about pediatrics? Because even with all the most wonderful information in the world – when working with kids, applying that can be really tricky. What if you don’t have a fancy biofeedback machine? What if you are not viscerally trained? What if children (or their parents) terrify you? As a teaching assistant, I received many calls, emails, and chats asking how to APPLY all that information, whether to their own kids or their patients.
If you are already an experienced pediatric therapist, this class is not for you. This class IS for the person who is a pelvic floor provider with pelvic floor skills but doesn’t know what the heck to do when a pediatric patient comes in to see them. This is for the therapist Pinterest-ing play skill ideas and asking on Facebook pelvic floor support groups how to make therapy something children and their parents buy into. It's for the person who wants to help little kids but just needs some basic skills and doesn’t have them in their toolbox. Maybe you’ve been a nanny, babysitter, auntie, or are a parent, but you just need to know what to do clinically.
Did you ever see those memes “do this thing but make it fashion.” Pediatric Pelvic Floor Play Skills embodies the idea of “do pelvic floor therapy with kids but make it look like we’re playing.” So, to set the expectations…there will not be standard biofeedback in this class and there also won’t be a ton of undressed or internal techniques because this is the starter toolbox.
What will be included?
-
- Manual techniques - can we teach a parent or child
- Positions - can we play to stretch or strengthen
- Extracurriculars - should we encourage
- How do we approach the colicky baby, the stubborn two-year-old, the chatter preschooler or even scarier…the TWEEN
- Managing a child’s care team at every age, stage and different settings
- Activity recommendations, toy suggestions with a purpose, resources for if you need more help
Not sure if this is for you? Here is some feedback from our last class:
“I’ve been a pediatric PT for 26 years and practiced in the home based, school and sensory gym settings primarily until making the jump over to hospital-based outpatient and NICU in the last seven. We’ve been developing the pediatric pelvic program, with the help of our adult pelvic therapists. I jumped in right away when I saw your course, as it seemed a natural progression from the PEDS 1 course that I attended under Dawn Sandalcidi. I was a little hesitant at the online format, as I know I don’t learn as well in that format as I do in person, but I was happily proven wrong. Mora was dynamic and really made the course lively and fun. Thank you for such a great course.”
“I want to start by saying I think it was a great course that was very well put together. I enjoyed the videos demonstrating with all the treatment techniques as I am a visual learner, and this was incredibly helpful.”
“I really enjoyed taking this course and felt that I learned a lot. The way Mora presented patient treatment videos/examples was very helpful.”
To learn more about Pediatric Pelvic Floor Play Skills join Mora in her upcoming course scheduled for March 24, 2024. If you miss the spring course, it is also scheduled for June 29th, and October 20th.

My name is Christina Trautman, and I am the Owner of The Pelvic Floor Place in Vancouver, WA. I am 39 years old and have been a practicing Pelvic Floor Physical Therapist for almost 14 years. I did not just stumble upon this career, it saved me.
I started having pelvic floor issues at the age of 7, peeing my pants when I would laugh. I had no physical trauma or incident as to why this was happening so as a 7-year-old, this was obviously humiliating and so embarrassing. This continued throughout elementary and went into middle school. When I was 13 and first got my period, I literally could not put in a tampon because my pelvic floor and vagina was so tight. This was frustrating and very inconvenient for an active sport-playing high schooler especially because all my friends could. What was wrong with me? I often felt alone and had no one I could talk to about my issues. After pleading with my mom to take me to a gynecologist for this difficulty and debilitating periods, I finally went as a sophomore in high school. It was the worst pain and experience of my life. Not only was I cramping for days and sobbing from the pain, but she told me, “You just need to have a kid and all your pain and issues will go away.”
Thankfully, I didn’t listen to her as getting pregnant at 14 wasn’t exactly the story I wanted and literally I probably couldn’t have sex if I tried. I continued to leak with laughing, couldn’t use a tampon, had debilitating periods, and was scared to death to date anyone. No one I knew had any of the same issues I had, and it wasn’t really a conversation my mom wanted to have with me. So, I continued to feel alone and in a lot of pain.
I compensated with my body throughout high school and college and couldn’t see improvement until I had Pelvic Floor Physical Therapy in my sophomore year in college. I was working as an aide in a PT clinic and luckily, they had a great Women’s Health PT there who noticed I had some pelvic floor symptoms. I was treated by her for a few years on and off and saw a huge improvement in my pain, leaking, and weakness. She connected the dots on all my issues that really stemmed from anxiety and an out-of-whack nervous system that started as a young kid after my parents divorced at the age of 3. After several treatments, I could put a tampon in, I didn’t leak with laughing, and was starting to get stronger in my core and pelvic floor.
I knew I had to go to PT school to treat women who had similar issues, so they too didn’t feel alone, embarrassed, humiliated, and frustrated.
My first job out of PT school was with that same therapist who treated me during college in Beaverton, OR. I took a Herman & Wallace Women’s Health class on a weekend before graduating from PT school and started studying all about the pelvic floor along with studying for my boards. She mentored me and I started seeing Women’s Health clients on day 1 of work. I loved it. This was my calling.
I split my time at that fast-paced office and a smaller clinic in Scappoose, OR. I was there for 2 years treating about 25-30% of women’s health clients. During that time, I took 3 different Herman & Wallace courses along with other classes dealing with Women’s Health. Every time I took a class, I wanted more. I wanted more complex clients and more time to treat them. I started dating a guy who lived in Vancouver WA, who is now my amazing husband, and I was ready for a change, so I took a job at a Chronic Pain clinic working as their Pelvic PT Specialist in Vancouver WA. I learned a ton and got to work with a good friend of mine. However, every day on my schedule, I would get so excited for my Pelvic clients and bored with my other orthopedic clients. So, I started looking for a full-time Pelvic PT position.
My best friend was working at a Pilates-based PT/Chiropractic office in Portland and they were looking for a Pelvic Floor PT. Despite the early morning hours and the long commute, I took the job. I was there for about 2 years and loved it. It was so fun working with chiropractors and skilled PTs. It was slow-paced but challenging and I was trained in Pilates Based PT. After getting pregnant, I decided the commute at 5 am to Portland was going to be too much so I took part-time jobs in Vancouver where I lived. This is when I opened my clinic.
I knew I always wanted to be a business owner; it was just so daunting. So, during my pregnancy, I slowly started seeing a couple of clients a week at my house while working part-time at other clinics in the area. This was amazing. I loved being in control of my own schedule and treating how I wanted to. I was mostly treating incontinence, prolapse, and pelvic pain but due to being pregnant, I started to get more interested in pregnancy and postpartum.
On December 25, 2017, I had my first baby, a 5-hour labor that I worked my tail off for. I had a great pregnancy and was highly active and ended up having a quick first vaginal birth with a very quick recovery. I owe that to all the exercises, breathing, and meditation I did during my pregnancy. I had a small tear with a natural vaginal birth but healed quickly with treatments I did on myself and was able to have sex within a few months with a supportive partner. Thinking about where I started to this point was miraculous. I did suffer from a grade 1 rectal prolapse about 5 weeks post-partum as I was struggling with constipation and a crying infant. As you can imagine, this was very frustrating as a Pelvic Floor PT, but those symptoms improved after I applied what I knew to my diet and exercises for my pelvic floor to help with strength and support. I owe all my success to having a supportive team to help me through my pelvic floor issues, pelvic floor PT, and a supportive partner. After recovering and getting back to work, I started taking more classes and getting certifications in pregnancy and postpartum classes. Ooh, this was my happy place. Starting to treat clients when the issues were really starting for most women was what I wanted to do.
I continued to slowly grow my business over the next few years as well as work at clinics in the area. It was a nice split. Enter my second pregnancy and covid. I had a great pregnancy and tried to keep as active as I could and the stress as low as I could. I had a 3-hour labor with no complications and a very fast recovery. How did I go from not being able to put a tampon in to delivering an 8 lb. baby without tearing? Pelvic PT is how! I truly was so proud and amazed at what my body could do. After I had Noah, I slowly started increasing my clientele and eventually decided to go full-time with my business.
During the last 5-6 years, I kept thinking about the Pelvic Rehab Practitioner Certification (PRPC) and kept putting it off for different reasons. After my son was about 2 and no longer requiring as much of my attention, I started studying for the test and passed in November of 2022. Woohoo!
I was still seeing clients at my house 4 days and week and in January of 2023 decided I needed to be in a real office. So, I joined forces with a prenatal chiropractor and a midwife group, and we opened up all 3 of our women-owned businesses in Felida, a small neighborhood and up-and-coming area near where I live. I am now mostly full-time, but I am as busy as I want to be while keeping a flexible schedule with the kids. I still have to work on my exercises and am aware of my pelvic floor, but I am no longer suffering with pain with sex, leaking, or weakness. I rewrote my story and yes while having kids did help (I will never tell that gynecologist that however), it really was Pelvic Floor Physical Therapy that has allowed me to live a normal life.
BIO:
Christina Trautman, PT, DPT, PRPC received her bachelor’s degree in Life Science from the University of Portland and her Doctorate in Physical Therapy from Pacific University. Through her personal experience with pelvic floor dysfunction and her extensive training, she found a passion for Women’s Health therapy and went on to take the Pelvic Floor Series courses (now Pelvic Function) through Herman & Wallace and holds her Pelvic Rehabilitation Practitioner Certification (PRPC).
Christina has been treating and aiding women with pelvic floor dysfunction for over 12 years and recently received her PRPC certification, making her one of the most sought-after pelvic floor rehab specialists in the area. She has also received her Postpartum Corrective Exercise Specialist Certification, Pre- and Post-Natal Corrective Exercise Specialist Certification, STOTT Rehab Pilates Mat and Reformer, and is pursuing more classes in pregnancy and postpartum care. She also treats orthopedic conditions and has a background in NAIOMT, ASTYM, and other manual therapy and exercise certifications.
Christina specializes in treating pregnancy and postpartum care, pain syndromes, pelvic organ prolapse, incontinence, and how to restore balance in the pelvic floor. She focuses on holistic care with a gentle approach to treating the pelvis and structures within the body that alter the mechanics of the pelvic floor. She also offers pregnancy and postpartum training programs.
Christina is the creator of The Pelvic Floor PlacePelvic Floor Place, and her desire is to treat women dealing with pelvic floor issues as well as helping pregnant and postpartum moms rehabilitate after having babies.
In her free time, she enjoys spending time with her family, getting outside, and enjoys working out with pilates, yoga, barre 3, and CrossFit.
Darla Cathcart, PT, DPT, Ph.D., WCS, CLT graduated from Louisiana State University (Shreveport, LA) with her physical therapy degree, performed residency training in Women’s Health PT at Duke University, and received her Ph.D. from the University of Arkansas Medical Sciences. Her dissertation research focus was on using non-invasive brain stimulation to augment behavioral interventions for women with lifelong vaginismus, and her ongoing line of research will continue to center around pain with intercourse. Darla is part of Herman & Wallace's core faculty and recently launched her own course Vaginismus and Vulvovaginal Dyspareunia. She sat down with the Pelvic Rehab Report to discuss working with vaginismus and vulvovaginal dyspareunia patients.
I believe one of the most important things that we as pelvic therapists can do for patients experiencing vaginismus and vulvovaginal dyspareunia is to offer HOPE!
These patients often arrive at therapy with a belief that something is uniquely wrong with them. Often, they have been to more than a handful of other doctors and care providers who are unfamiliar with pelvic floor problems causing pain with sex (which is substantiated by the research) who have maybe given them messages of "I can't find anything wrong with you" and "You just need to relax."
If I had a dollar for every time a patient told me that another care provider told them to "Just drink a glass of wine before sex to help you relax" (palm to forehead!)...These messages often cause these patients to feel as if their pain with sex is made up in their heads, or that a scary diagnosis is being overlooked.
Unfortunately, unless they have found a provider who can quickly identify that the patient has a musculoskeletal problem with the pelvic floor that needs a pelvic therapy referral, then the patient has often gone for many months, years, or even a decade or more without being properly heard or getting the right help.
When I sit down with a patient, after hearing a bit of that person's story, I typically start the conversation with "Thank you for sharing your story. I want you to know that you are not alone - a big percentage of my patients have pain with sex. I also want you to know that based on what you are telling me, you will likely get better as most of them have done."
Patients often express relief, sometimes disbelief, or both, mixed with some hope - a bit of "Ah, this person hears me and knows what I'm talking about, and says I can get better!" The belief of being able to get better, even if mixed with some doubt, is an extremely valuable start on their healing journeys.
There are many factors that the pelvic therapist could consider to facilitate conversations around pain with sex.
As with all of our patients seeking pelvic rehab, communication requires non-judgment and respecting a patient's boundaries. Asking a patient "Have you been sexually abused or had sexual trauma in the past?" can feel unnerving and alarming for a patient who is not ready to have that conversation with their pelvic therapist. However, asking a patient "Have you had any negative sexual experiences that you would like to share, that you feel may be impacting your symptoms?" allows the patient to decline until they feel ready to engage in such a conversation.
This softer approach lets the patient know that the therapist is open to a conversation about impactful events and respects that patient's autonomy in sharing that history. Putting the patient in the driver's seat is also critical. For instance, consider a patient who, theoretically, would benefit greatly from using vaginal trainers (dilators) but declines to use them. An approach of "but using trainers will be the only way to get better" may result in the patient quitting therapy, or worse, feeling traumatized from the therapy experience. Alternatively, affirming to patients that the treatments chosen are their prerogative keeps the path for ongoing healing and provider trust.
A statement of "Not using vaginal trainers is your choice, but we can always consider them again in the future if you change your mind. Let me talk you through the alternative treatments, and how their effects will differ from that of the vaginal trainer use" leaves the door open to return to that treatment down the road if the patient chooses, and also respects the choice of the patient in the moment. The key is to not be pushy about pursuing the undesired treatment down the road! It could be mentioned again, but use judgment and caution in the approach.
A final highlight is being sure to give patients space to share their story, as often they have not been heard by previous providers or their symptoms have been discounted.
My course Vaginismus and Vulvovaginal Dyspareunia, is scheduled for March 3rd and September 14th this year and takes a deep dive into the detail of how to make the rubber meet the road to not only get treatment started but to really help progress a patient into a satisfying sex life. This course was developed so that the participant could leave this course and understand how to really approach the examination, history taking, and step-by-step procedures in instructing and using vaginal trainers and other tools for patients having painful intercourse. Additionally, this course should increase the practitioner's confidence in incorporating instructions and education related to a patient's concerns about the female sexual cycle and response (arousal, desire, orgasm), sexual positioning, lubrication, and partner integration.

There are currently two scheduled course offerings available for Modalities and Pelvic Function: Philadelphia PA in April 6-7 and Manchester NH in August 24-25. If neither of these work for your location or schedule then consider hosting! The hosting requirements and interest form can be found on the Host a Course page.
The new Modalities and Pelvic Function - Pelvic Health Clinical Toolkit is an in-person two-day continuing education course targeted to pelvic health clinicians covering frequently used modalities in pelvic health, including biofeedback and EStim. This course was designed to answer the clinician’s need to understand how to choose and access the right tools, both for in-clinic care and for patient self-care application.
One of the course co-creators, Mora Pluchino shared “This class will be unlike one you've taken before. The H&W curriculum team sat down and thought about how we could make this the most interactive, hands-on, and practical course while still staying evidence-based and professional. This will be an in-person learning opportunity with 2 days of lab, demonstration, and interactive learning opportunities. If there is a modality that exists in pelvic health, it will likely have a debut here. This class is made for anyone who wants to learn to apply modalities in the variety of uses possible for pelvic health!"
Biofeedback and electrical stimulation are covered in this course, as are introductions to understanding tools such as shockwave, dry needling, real-time ultrasound, laser, and electrotherapies. With hands-on lab time and learning modules grouped into tools specific to pelvic health conditions such as bowel dysfunction and sexual health challenges, practitioners will have the opportunity to trial various tools and applications that previously may have only been available as an image in a presentation.
When our popular Pelvic Function Level 1 course, which introduces participants to the world of pelvic health, was transitioned to a satellite lab course one of the content pieces that was left out was the modalities focus - simply because the equipment was too difficult to ship to multiple satellite locations around the country. Herman & Wallace is thrilled to announce that not only have we solved this issue, but designed a way for clinicians to learn about dozens of modalities in an environment that allows the clinician to move beyond theoretical and soundly into the practical delivery of a variety of technologies and tools.
Current Medical Technologies will be in-person with us as we design this learning experience and will be available to answer your questions about products and clinical set-up. The interactive environment has been designed to be stimulating and allow the clinician to apply a variety of learning strategies including tactile opportunities to try things on themselves or a lab partner. This is a unique course that provides a foundational understanding of technology and tools, clinical practice research, and recommendations in an in-person environment. Many equipment providers have been generous in providing sample products for trial and even some giveaways to take home!
We believe this Modalities course is so foundational to our skillset in pelvic health that we have added it to our core Pelvic Function Series. This course is intended to be taken after Pelvic Function Level 1 and can be taken at any point following the introductory course as you work your way through the PF Series. If you’re wondering “When should I take this course?” the answer is “as soon as you can!”
Nari Clemons, PT, PRPC has written the following courses: Lumbar Nerve Manual Assessment/Treatment, as well as Sacral Nerve Manual Assessment/Treatment. She has co-authored the Pelvic Function Series Capstone course and the Boundaries, Self Care, and Meditation Course. Nari’s passions include teaching students how to use their hands more receptively and precisely for advanced manual therapy skills while keeping it simple enough to feel successful. She also is an advocate for therapists learning how to feel well and thrive as they care for others, which is a skill that can be developed.
If you've taken the Pelvic Function Series Capstone or Pelvic Function Level 2B and you've gotten curious about nerves, you've likely started to think about what is nerve pain and what is muscle restriction. In those classes, we discuss several lumbar nerves and how the restrictions could be creating pain in the anterior vulva, anterior hip, lower abdomen, groin, or inner thigh. Or perhaps you've started to notice certain patients have pain along nerve distributions we talk about in either of those courses. Sometimes we have patients who have had surgeries like c-sections, inguinal hernia repairs, or hysterectomy, and we notice they are having a persistent pain or weakness problem that isn't easily explained through muscle alone. I like to think of the nerve as the program for the robot, and the muscle as the way the robot moves. Nerves are a way to get deeper to the root of what may be happening.
We have separate classes for the Lumbar Plexus Nerves (ilioinguinal, iliohypogastric, genitofemoral, obturator, femoral, and lateral femoral cutaneous) and the Sacral Plexus (pudendal, sciatic, inferior and superior gluteal, and the posterior femoral cutaneous nerves). Here is a clinical example of each Lumbar nerve and some differential cues we may look for, that we may have mistaken for muscle in the past:
Iliohypogastric: an area of pain or weakness, unilateral, or an outpouching in the obliques, a diastasis abdominus that you are treating where the patient continues to have difficulty recruiting the transverse abdominus in the area near the c-section.
Ilioinguinal: a persistent pain in the pubic bone region after pregnancy or high groin pain ( if x-rays do not confirm osteitis pubis). Also, pain in the labia majora or testicle.
Obturator: a pain in the inner thigh, or often after a transvaginal tape (bladder sling), even years later, as the sling goes through the obturator foramen, which can tighten over time, creating pain. This can also be persistent adductor tightness and tenderness that is not consistent with other muscle groups.
Genitofemoral: a pain in the anterior vulva or clitoral area that can also feel like persistent burning or itching (when a dermal condition has been ruled out). This is often called vulvodynia (which just means pain in the vulvar area), but it can be differentiated from pudendal pain in that it is not worse when sitting and is limited to the anterior vulva.
Femoral: a weakness in one quad, a leg that occasionally gives out when stepping off a curb unilaterally, a hip flexor that stays tighter than the other side, despite stretching, often mistaken for "psoas dysfunction"
Lateral femoral cutaneous nerve: meralgia paresthetica: numbness in the outer thigh after pregnancy or LFC injury, or patients will describe feeling like there is a jean seam rubbing the outside of their leg when there isn't, also persistent IT band pain or stiffness.
If nerves are of interest to you, come join us for Lumbar nerve manual assessment and treatment, and learn how to treat nerves from proximal to distal, differentially diagnose more, how to decompress the pathway of the nerve, and then restore the affected structures to normal length and strength.
If you would like to learn more about Lumbar Nerve Manual Assessment and Treatment the join Nari in her upcoming course on March 2-3, 2024.
By accepting you will be accessing a service provided by a third-party external to https://www.hermanwallace.com/
All Upcoming Continuing Education Courses



Pelvic Function Level 1 - In-Person - Greensboro NC - June 7 - 8 2025 - SOLD OUT
Jun 7 2025 - Jun 8 2025

Nutrition Perspectives for the Pelvic Rehab Therapist - Remote Course - June 7 - 8 2025
Jun 7 2025 - Jun 8 2025





Pelvic Function Level 1 - Satellite - Torrance CA - June 14 - 15 2025 - SOLD OUT
Jun 14 2025 - Jun 15 2025

Pelvic Function Level 1 - Satellite - Long Beach CA - June 14 - 15 2025 - SOLD OUT
Jun 14 2025 - Jun 15 2025

Pelvic Function Level 1 - Satellite - Woodbury NY - June 14 - 15 2025 - SOLD OUT
Jun 14 2025 - Jun 15 2025


Pelvic Function Level 1 - Satellite - New York NY - June 14 - 15 2025 - SOLD OUT
Jun 14 2025 - Jun 15 2025

Pain Science for the Chronic Pelvic Pain Population - Remote Course - June 21 - 22 2025
Jun 21 2025 - Jun 22 2025

Dry Needling and Pelvic Health - In-Person - Atlanta GA - June 21 - 22 2025 - SOLD OUT
Jun 21 2025 - Jun 22 2025



Mobilization of Visceral Fascia - Gastrointestinal - Satellite Lab Course - St. Petersburg FL - June 27 - 29 2025
Jun 27 2025 - Jun 29 2025

Mobilization of Visceral Fascia - Gastrointestinal - Satellite Lab Course - Self-Hosted - Jun 27 - 29 2025
Jun 27 2025 - Jun 29 2025

Mobilization of Visceral Fascia - Gastrointestinal - Satellite Lab Course - Sellersville PA - June 27 - 29 2025
Jun 27 2025 - Jun 29 2025

Mobilization of Visceral Fascia - Gastrointestinal - Satellite Lab Course - Milwaukee WI - June 27 - 29 2025
Jun 27 2025 - Jun 29 2025

Mobilization of Visceral Fascia - Gastrointestinal - Satellite Lab Course - Medford OR - June 27 - 29 2025
Jun 27 2025 - Jun 29 2025

Mobilization of Visceral Fascia - Gastrointestinal - Satellite Lab Course - Bartlett IL - June 27 - 29 2025
Jun 27 2025 - Jun 29 2025

Mobilization of Visceral Fascia - Gastrointestinal - Satellite Lab Course - Cedar Knolls NJ - June 27 - 29 2025
Jun 27 2025 - Jun 29 2025

Mobilization of Visceral Fascia - Gastrointestinal - Satellite Lab Course - Marysville OH - June 27 - 29 2025
Jun 27 2025 - Jun 29 2025

Mobilization of Visceral Fascia - Gastrointestinal - Satellite Lab Course - New Orleans LA - June 27 - 29 2025
Jun 27 2025 - Jun 29 2025

Mobilization of Visceral Fascia - Gastrointestinal - Satellite Lab Course - Albany NY - June 27 - 29 2025
Jun 27 2025 - Jun 29 2025

Mobilization of Visceral Fascia - Gastrointestinal - Satellite Lab Cource - Amherst OH - June 27 - 29 2025
Jun 27 2025 - Jun 29 2025

Mobilization of Visceral Fascia - Gastrointestinal - Satellite Lab Cource - Paso Robles CA - June 27 - 29 2025
Jun 27 2025 - Jun 29 2025

Mobilization of Visceral Fascia - Gastrointestinal - Satellite Lab Course - Detroit MI - June 27 - 29 2025
Jun 27 2025 - Jun 29 2025



Pelvic Function Level 1 - Satellite - Tampa FL - June 28 - 29 2025 - SOLD OUT
Jun 28 2025 - Jun 29 2025


Pelvic Function Level 1 - Satellite - Waco TX - June 28 - 29 2025 - SOLD OUT
Jun 28 2025 - Jun 29 2025



Pelvic Function Level 1 - Satellite - Milwaukee WI - July 12 - 13 2025 - SOLD OUT
Jul 12 2025 - Jul 13 2025

Modalities and Pelvic Function - In-Person - Houston TX - July 12 - 13 2025
Jul 12 2025 - Jul 13 2025
Pelvic Function Level 1 - Satellite - Denver CO - July 12 - 13 2025 - SOLD OUT
Jul 12 2025 - Jul 13 2025

Pelvic Function Level 2B - Satellite - Sellersville PA - July 19 - 20 2025
Jul 19 2025 - Jul 20 2025