

Do you feel you lack a firm understanding of how to comprehensively treat pregnant and postpartum athletes? Maybe you don’t feel confident in knowing how to modify activity for this population, or you feel that most high-intensity activity should be ceased during pregnancy and early postpartum.
If this is you, might I encourage you to take our upcoming course on special considerations for Pregnant and Postpartum High-Intensity Athletes?
While this patient population is like the general population in many ways, there is a certain nuance in evaluating pregnant and postpartum athletes. This is especially true for elite or high-intensity athletes. Considering the demands of many of these high-intensity sports (running, powerlifting, CrossFit, Orange Theory) it is imperative that pelvic therapists also understand orthopedics, and vice versa. In bridging this gap between specialties, we have the opportunity to optimize performance, while ensuring our patients also remain healthy.
Keeping this in mind, our evaluation will look a bit different than traditional pelvic and orthopedic evaluations. Specifically, each respective specialty should be screening the other. If you are a pelvic therapist, you should also be screening the lumbar spine, SI joint, Hip joint, and mid-thoracic spine. You should also be performing a functional movement analysis that is specific to their desired sport. If you are an orthopedic therapist, you should also be screening for diastasis recti, pressure management capability, and pelvic floor tension and/or weakness. While orthopedic therapists will not be performing an internal exam like their pelvic therapist counterparts, there are still several screening methods that can be used to determine if a patient requires referral to a pelvic PT. And that is exactly what this course aims to do.
Pregnancy and Postpartum Considerations for High-Intensity Athletics aims to bridge the gap between pelvic and orthopedic therapists and to help educate providers on how to evaluate this patient population with confidence. We will cover special medical considerations for this patient population, ways in which to modify activity for this population, and how to keep them doing what they love safely throughout pregnancy and postpartum. So, if you would like to learn more about working with pregnant and postpartum athletes, go ahead and sign up for our September 15th course offering. We’d love to have you!
AUTHOR BIO
Emily McElrath PT, DPT, MTC, CIDN
 Emily McElrath is a native of New Orleans and received her undergraduate degree in Athletic Training at the University of Southern Mississippi and went on to receive her Doctorate of Physical Therapy from the University of St. Augustine for Health Sciences. She is highly trained in Sports and Orthopedics and has a passion for helping women achieve optimal sports performance. Emily is certified in manual therapy and dry needling, which allows her to provide a wide range of treatment skills including joint and soft tissue mobilization. She is an avid runner and Cross-fitter and has personal experience modifying these activities during pregnancy and postpartum. While not working, Emily enjoys time with her husband and two kids.
Emily McElrath is a native of New Orleans and received her undergraduate degree in Athletic Training at the University of Southern Mississippi and went on to receive her Doctorate of Physical Therapy from the University of St. Augustine for Health Sciences. She is highly trained in Sports and Orthopedics and has a passion for helping women achieve optimal sports performance. Emily is certified in manual therapy and dry needling, which allows her to provide a wide range of treatment skills including joint and soft tissue mobilization. She is an avid runner and Cross-fitter and has personal experience modifying these activities during pregnancy and postpartum. While not working, Emily enjoys time with her husband and two kids.


I arrived to Pelvic Health Physical Therapy by fruitful exposure and a professional demand to fulfill a new employer’s needs. 10 years later, I am all-in serving women and men with bladder, bowel, sexual dysfunction, and abdominopelvic pain to optimally live their lives well more comfortably.
Throughout my PT education at Washington University in St. Louis, I envisioned specializing in Orthopedics using a Movement Systems Impairment (MSI) diagnostic and treatment approach. While a student in my final 3-month clinical experience at a hospital-based Outpatient Orthopedic Clinic, I had the good fortune to be paired with a clinical instructor who was largely Orthopedic-based but treated Pelvic Health 1 day per week as the sole Pelvic Health PT Provider (shoutout Barb Davis!). The setting was a large community-based safety-net institution, Denver Health, which served Denver residents including underserved populations. Patients presented with chronic pain, complex socioeconomic dynamics, and diverse ethnic backgrounds with Denver historically being a migrant and refugee-welcoming city. My pelvic patients were interesting, and my Pelvic Health interest was sparked.
As a new graduate seeking employment, I secured a job at a hospital-based Outpatient Orthopedic Clinic in San Diego, CA at Scripps Health. My new position was created for an Orthopedic PT who was interested in being mentored in Pelvic Health PT due to a growing need to support Pelvic Health patients and providers in North County San Diego. I was offered mentorship and financial support to pursue continuing education to set a foundation in Pelvic Health. I had an interest, there was a clinical need, I seized the opportunity, ran with it, and I am so grateful I did.
My astute Pelvic Health Mentors (Alissa Meredith, PT, MPT and Destiny Bochinski, PT, DPT, PRPC) highly encouraged me to take the foundational Pelvic Floor Series (which has been updated to the Pelvic Function Series this year) through Herman & Wallace. I was already familiar with Herman & Wallace through my exposure at Washington University in St. Louis, where they host various Herman & Wallace courses. I am so glad I chose to follow my Pelvic Health educational path with Herman & Wallace Rehabilitation Institute. I was lucky enough to be taught Pelvic Floor Level 1 (now called Pelvic Function Level 1) by the venerable and entertaining Holly Herman & Kathe Wallace. Fast forward 10 years and I have taken the full Pelvic Floor Series, Ramona Horton’s Visceral Fascia Mobilization Series, Male Pelvic Health, Nutritional Perspectives, Pregnancy Course, IC, Rehabilitative Ultrasound, and a myriad of other Herman & Wallace continuing education courses. I have a wide arsenal of didactic information, manual skills, proficiency in biofeedback modalities use, and clinical experiences to treat the gamut of simple to complex pelvic and orthopedic patients. Citing the incredible Ramona Horton, MPT, DPT, I completely agree that Pelvic Health is applying Orthopedics within the pelvic cavity. I am grateful to have a practice that is largely Pelvic Health-based with a smattering of Orthopedics. In reality, I practice ~65-70% Pelvic Health and 30-35% Orthopedics.
Across my professional journey, I started as the third Pelvic Health PT at the clinic where I work, to now being one of eight Pelvic Health PT providers at that same comprehensive outpatient rehab center, Scripps Rehabilitation Services in Encinitas. I am lucky to be part of a burgeoning Pelvic Health Team at our clinic site as well as across the larger health system. I was lucky to be mentored by two amazing colleagues, including now a Herman & Wallace Instructor, Destiny Bochinski, who I continue to work with and collaborate well with. I am appreciative of the opportunity to continue to grow professionally by serving as a Pelvic Health mentor at my clinic and TA for Herman & Wallace, which I’ve been doing since 2020.
Thank you for letting me share my story, which is one of seizing a ripe opportunity and allowing my career path to evolve with an initial spark that I didn’t early on envision would be my path, but I love where I’ve been and my trajectory forward.
AUTHOR BIO
Jackie Castillo, PT, DPT, MSC
 Jackie Castillo, PT, DPT, MSCI is a Board-Certified Orthopedic Clinical Specialist based out of San Diego, CA who practices Pelvic Health and Orthopedic Physical Therapy at Scripps Rehabilitation Services in Encinitas. She received her DPT and MSCI (Master of Science in Clinical Investigation) Degrees from Washington University in St. Louis in 2013. She received her BS in Animal Physiology & Neuroscience from the University of California, San Diego in 2005. She has served as a Teaching Assistant for Herman & Wallace since 2020. She intends to sit for the Herman & Wallace PRPC Exam this year. She enjoys running, yoga, walking her puppy, hiking, biking, and exploring good food and drink with her soon-to-be husband, family, and close friends.
Jackie Castillo, PT, DPT, MSCI is a Board-Certified Orthopedic Clinical Specialist based out of San Diego, CA who practices Pelvic Health and Orthopedic Physical Therapy at Scripps Rehabilitation Services in Encinitas. She received her DPT and MSCI (Master of Science in Clinical Investigation) Degrees from Washington University in St. Louis in 2013. She received her BS in Animal Physiology & Neuroscience from the University of California, San Diego in 2005. She has served as a Teaching Assistant for Herman & Wallace since 2020. She intends to sit for the Herman & Wallace PRPC Exam this year. She enjoys running, yoga, walking her puppy, hiking, biking, and exploring good food and drink with her soon-to-be husband, family, and close friends.

Sarah Clampett, PT, DPT, is Head of Clinical Operations at Origin, a leading provider of pelvic floor and whole-body physical therapy with a special focus on pregnancy and postpartum. After studying Kinesiology and Psychology at the University of California, Sarah stayed on to earn her Doctorate of Physical Therapy. As a clinical leader at Origin, she’s as passionate about helping PTs love the work they do as she is helping patients feel good in their bodies.

Shortly after I started physical therapy school, I realized that being a physical therapist is a fantastic conversation starter. People’s eyes tend to light up when they hear I’m a PT because almost everyone has had an experience with physical therapy — and even if they haven’t, they’ve had an injury. They want to tell me about the physical therapy they did in high school for their scoliosis or that time they tore their ACL skiing. They even seek advice for that pesky low back pain that hasn’t fully resolved since throwing their back out six months ago.
I love to hear people’s stories and genuinely enjoy engaging in casual conversations about injuries. When I’m done explaining that core strength is important when dealing with back pain, I go on to say that while I started my career in ortho, I’m now a pelvic floor PT. That’s when one of two things happens: 1) They stare at me blankly, then quickly change the subject, or 2) Their eyes light up even brighter and they start asking questions. That’s when the conversation gets really fun. “What exactly do you do?” “What do you treat?” and “How did you get into that?”
Where My Passion for Ortho Started
I decided to go to PT school for a couple of reasons. I’ve always loved sports and consider sports a large part of my upbringing. (Fun fact: I only listened to AM sports radio until I was about 13). And, like many PTs, I discovered physical therapy as a patient. In my case, it was after injuring myself in high school playing volleyball.
I loved going to PT, not only because I was getting better — I loved seeing all the other patients getting better around me. It was a very sports-oriented PT clinic and my first and only experience with PT, so when I declared Kinesiology as my major and started my pre-PT coursework in college, I had my heart set on being a sports/ortho PT. It felt like the perfect fit at the time. I was a student athletic trainer for 2.5 years in college to learn as much as I could about the sports rehab world before heading into PT school.
Fast forward to my final semester and clinical rotation at PT school: I was at an ortho clinic with a large population of athletes. I loved it. After I graduated, I was hired as a PT at that same clinic and started my career as a working PT. I began working a few days a week to build my caseload with the plan to transition to full-time as my schedule filled. That clinic happened to also own a women’s health clinic that treated primarily prenatal and postpartum patients. A few weeks after starting, I was asked if I wanted to work additional days by filling in at the women’s health clinic. As a new grad who needed to pay rent, I said yes because more days meant more money. It was supposed to be temporary.
My Journey to Becoming a Pelvic Floor PT
As soon as I walked into the women’s health clinic, something clicked. I fell in love with the patient population and helping them feel better. I remember early on, a patient with such severe pelvic pain that they could barely walk to the bathroom. At their next visit, they said they could walk without pain again. The ability to help people going through pregnancy and postpartum felt especially meaningful. I spent a year and a half working in both clinics and then transitioned to treating women’s health full time.
After working in women’s health for a couple of years, I eventually got tired of referring my patients with pelvic floor conditions to colleagues who treated pelvic floor and decided it was time to start treating it myself. To be honest, I was hesitant at first and definitely nervous about taking my first course. But as soon as I started treating the pelvic floor, something clicked again.
Even more so than in the past, I connected deeply with my patients and their goals. Giving someone the confidence to leave the house without wearing a maxi-pad or carrying extra underwear because they’re no longer worried about leaking was amazing. So many people suffer in silence from pelvic floor disorders and are resolved to just live with them. I’m lucky enough to provide a safe space to talk about it and assure them that it can get better. How cool is that?
Advice for an Ortho PT Curious About Pelvic floor
Take a course! Just because you take the course does not mean you are committing to a career change. Even if you decide it’s not the right time to switch or you didn’t enjoy it as much as you thought you would, you’ll still learn valuable information that you can immediately incorporate into your practice. That overworked, stressed patient with lingering hip pain might need pelvic floor lengthening to get that last bit of pain to resolve.
Most ortho PTs who make the shift are nervous they won’t be able to use their ortho skills when treating the pelvic floor, and that simply isn’t true. My time in ortho has definitely shaped the pelvic floor PT I am today.
In ortho, you treat the whole body. If your foot hurts, you look at the knee, the hip, the low back, and how everything works together to figure out what’s causing the foot pain. Pelvic floor PT is no different. You must look at the whole body and figure out how all the parts are working together to get the results you need. I continue to use many of the same exercises now that I used back when I was working as an ortho PT.
Lastly, the pelvic floor is a group of muscles. If it’s weak, it needs to strengthen. If it’s overactive, it needs to lengthen. If it’s uncoordinated, it needs to be retrained. Yes, treating pelvic floor dysfunction requires special training, but at the end of the day, muscles are muscles.


This blog contains an interview with Alyson N Lowrey, PT, DPT, OCS. Alyson treats the pelvic floor patient population through an orthopedic approach, working closely with pelvic floor specialists. Alyson’s clinical interests include evaluation/treatment of chronic pain, lumbar and cervical spine disorders, foot and ankle disorders, pelvic pain, and clinical instruction. Alyson is the co-instructor for the new H&W course, Pain Science for the Chronic Pelvic Pain Population - Remote Course scheduled for July 17-18, 2021.
Q: Who are you? Describe your clinical practice.
A: I work in an outpatient hospital-based clinic where I am able to provide true 1:1 care to patients of all ages and orthopedic conditions. Since pelvic floor therapy came to our clinic, I have developed strong clinical and personal relationships with pelvic floor therapists. We have been able to successfully combine our respective expertise into a wholistic approach for improving patient’s functional outcomes. My knowledge and relationships with pelvic floor therapy have allowed me as an ortho clinician to recognize when a patient’s dysfunction may have a pelvic floor component and refer appropriately. I am also in a unique opportunity where my pelvic floor colleagues will co-treat or transition care of a patient to me to continue to improve their overall function by providing functional strengthening and neuromuscular re-education to the pelvic floor musculature and other supportive muscular systems. This relationship also allows us to treat comorbid orthopedic conditions and pelvic dysfunctions such as low back pain or SIJ dysfunction as well.
Q: How did you get involved in the pelvic rehabilitation field?
A: I became involved with pelvic rehabilitation through working in a clinic with Tara Sullivan. Her knowledge is immense and our working relationship has shaped and changed how I assess patients. My practice has expanded drastically knowing so much more about pelvic floor dysfunction. I also have personal struggles with pelvic pain, which has given me a patient’s perspective as well on how important pelvic rehabilitation is.
Q: If you could get a message out to other clinicians about pelvic rehab what would it be?
A: I would encourage all ortho clinicians to educate themselves on pelvic rehab. Pelvic rehab is not yet fully integrated into our DPT curriculums and is often treated as a very separate area of dysfunction. Integrating pelvic floor function and dysfunction into my ortho world has drastically changed how I see and treat many patients.
Q: What made you want to create this course, Pain Science for the Chronic Pelvic Pain Population?
A: Tara and I wanted to create this course to help other clinicians become more proficient at treating chronic pain. A large portion of our caseloads is chronic pain both generally and with pelvic conditions. Patients with these conditions are often overlooked and not treated appropriately by the medical system at large. They are often dismissed or mislead that they have something drastically wrong with them, or worse, nothing wrong with them at all. This population often has the most functional deficits and the worst clinical outcomes. We want to change that.
Q: What need does your course fill in the field of pelvic rehabilitation?
A: There is a need in rehabilitation and medicine to understand pain from a biopsychosocial approach and to treat chronic pain conditions from that perspective. Pain is complex, and treatment is complex. Chronic pelvic pain is a subdivision of prevalent chronic pain that is not talked about or treated often enough.
Q: Who, what demographic, would benefit from your course?
A: Any clinician who treats chronic pain conditions can benefit from this course.
If you would like to learn more about chronic pelvic pain, you can join Alyson at Pain Science for the Chronic Pelvic Pain Population - Remote Course scheduled for July 17-18, 2021.

Leg length discrepancy (LLD) is when there is a noticeable difference in length of one leg to the other. LLD is common and can be found in 70% of the population (Gurney, 2002). LLD can be structural or functional. Structural LLD is when a long bone in the leg is longer or shorter than the other. Structural LLD is often the result of congenital or boney damage of epiphyseal plate. Functional is when there is an apparent LLD from higher in the chain such as scoliosis. Generally as pelvic floor therapists we are orthopedic based therapists. In physical therapy school we learned that a leg length discrepancy had to be >1 cm to be considered significant, and based off of recent research that is still the case. Research in the last few years has focused on whether LLD has an effect on age related changes with osteoarthritis, posture & gait, and pain. Physiopedia suggests differential diagnosis of sacroiliac dysfunction, scoliosis, low back pain, iliotibial band (ITB) syndrome, stress fractures, and pronation. It can often feel like a chicken or egg question.
 In the clinic I typically screen for a leg length discrepancy during my initial evaluation. A LLD may be noticed upon observation of gait assessment, standing posture, or part of the pelvic obliquity screen in standing and then in supine.
In the clinic I typically screen for a leg length discrepancy during my initial evaluation. A LLD may be noticed upon observation of gait assessment, standing posture, or part of the pelvic obliquity screen in standing and then in supine.
During gait, a LLD will create bilaterteral gait impairments. Khamis et al did a systematic review of LLD and gait deviations in 2017. They narrowed the search down to 12 articles and found that LLD >1cm was significantly related to gait deviations. These deviations occurred bilaterally, and while initially compensations occurred in the sagittal plane, as the LLD increased so did the gait deviations, and then affected frontal planes of motion as well. Resende et al (2016) agrees that even mild LLD should not be overlooked. They found that the most likely gait deviations were also in the sagittal planes and consisted of rearfoot and ankle dorsiflexion and inversion, knee flexion and adduction, hip adduction and flexion, and pelvic trendelenburg.
The sagittal, or right/left plane, and frontal, or front/back, plane involvement is consistent with the differential diagnosis of sacroiliac dysfunction, low back pain, and pronation. Really, one could justify why a LLD could contribute to pain and dysfunction in most of the lower body. It is reasonable to think that these compensational moments in gait over a long period create boney changes in the lower extremities which may contribute to low back pain.
Clinically, a leg length discrepancy can be assessed directly with a tape measure or indirectly with a shoe lift. Badii (2014) found a higher interrater reliability with the indirect method of a shoe lift as opposed to measuring with a tape measure.
Rannisto et al (2019) looked at leg length discrepancy among meat cutters with low back pain. All participants had been working for 10 years and were greater than 35 years old. Participants needed to have a LLD of 5mm (5mm is 0.5 cm) or more and complain of low back pain of >2/10 on visual analog scale (VAS). They were all given insoles and randomized into 2 groups; the intervention group were given lifts to correct the LLD about 70%; for example a 10mm LLD was corrected to 3 mm. The LLD was measured with a laser ultrasound technique. Participants were followed for 12 months. The intervention group had improvement in low back pain intensity, sciatica intensity, and took less sick time. Possibly the most amazing part is that for those that wore the heel lift at work the compliance was good.
Leg length discrepancy can often be an underlying component contributing to complaints of pain and dysfunction. It may have more of an effect on the populations who stand or walk for most of their work, and I wonder as more people transition to standing desks if we will see more people come into the clinic with a previously undiagnosed LLD.
My biggest clinical pearls from this research is that:
- Heel lifts can be used to diagnose and then for treatment (yay! One less step of getting the tape measure out)
- The heel lift does not have to be perfect. Clinically, I will try a lift and have the person walk, and then we can make a team decision if this lift is enough and feels better
- The gait compensations are consistently adduction and internal rotation throughout the lower body chain. I will continue to work on the opposing muscle groups; lateral rotators, hip extensors and abductors.
Leg Length Discrepancy can be evaluated using various assessments. To learn orthopedic evaluative techniques for patients, consider joining Lila Abbate in her course Advanced Orthopedic Assessment for the Pelvic Health Therapist.
Maziar Badii, A Nicole Wade, David R Collins, Savvakis Nicolaou, B Jacek Kobza, Jacek A Kopec, Comparison of lifts versus tape measure in determining leg length discrepancy; Journal of Rheumatology 2014, 41 (8): 1689-94
Renan A. Resende, Renata N. Kirkwood, Kevin J. Deluzio, Silvia Cabral, Sérgio T. Fonseca. "Biomechanical strategies implemented to compensate for mild leg length discrepancy during gait" Gait & Posture, Volume 46, 2016; 147-153, https://doi.org/10.1016/j.gaitpost.2016.03.012
Sam Khamis, Eli Carmeli, Relationship and significance of gait deviations associated with limb length discrepancy: A systematic review, Gait & Posture, Volume 57, 2017, 115-123, https://doi.org/10.1016/j.gaitpost.2017.05.028
Burke Gurney, Leg length discrepancy, Gait & Posture, Volume 15, Issue 2, 2002, Pages 195-206, https://doi.org/10.1016/S0966-6362(01)00148-5.
Satu Rannisto, Annaleena Okuloff, Jukka Uitti, et al. Correction of leg-length discrepancy among meat cutters with low back pain: a randomized controlled trial. BMC Musculoskeletal Disorders. 2019;(1):1. doi:10.1186/s12891-019-2478-3.

How does a male sports and orthopedic physical therapist come to teach about pelvic health and wellness? I was fortunate enough to spend ten years in the NHL as the physical therapist and athletic trainer for the Florida Panthers. Ice hockey is one of the sports that has the highest incidence of groin strains among other pelvic related pathologies.1 As a clinician that was responsible for taking care of the world’s best hockey players, I was challenged to understand the interconnected relationships between the lumbopelvic-hip complex very quickly.
 In the early years of my career development and the treatment of mostly males with pelvic pathologies, I leaned heavily on pelvic health professionals to help me understand an area of the body I received little training on in school and even less in my clinical care as a sports and orthopedic manual physical therapist. After years of treating hip and pelvic pathologies on my players I became more comfortable in this enigmatic area of the body. A good friend of mine was on faculty with Herman & Wallace and we frequently would communicate and compare notes. She was treating an increasing number of “sports hernias” (now termed athletic pubalgia or core muscle injury) and was relying on me to help her understand this injury and how to treat it. In turn, she helped me understand what went on in the pelvic health profession and what those therapists were trained to treat and how they went about it.
In the early years of my career development and the treatment of mostly males with pelvic pathologies, I leaned heavily on pelvic health professionals to help me understand an area of the body I received little training on in school and even less in my clinical care as a sports and orthopedic manual physical therapist. After years of treating hip and pelvic pathologies on my players I became more comfortable in this enigmatic area of the body. A good friend of mine was on faculty with Herman & Wallace and we frequently would communicate and compare notes. She was treating an increasing number of “sports hernias” (now termed athletic pubalgia or core muscle injury) and was relying on me to help her understand this injury and how to treat it. In turn, she helped me understand what went on in the pelvic health profession and what those therapists were trained to treat and how they went about it.
This collaboration eventually led to me joining Herman & Wallace and offering a sports and orthopedic perspective to pelvic floor consideration. I have attended Herman & Wallace’s Pelvic Floor courses to fully understand the training that a pelvic health therapist undergoes. Admittedly, I do not perform internal work because I have found a niche helping clinicians such as myself who understand that the pelvic floor is a key variable in human movement and we need to understand it at a much higher level than what we are exposed to in school, but don’t have the career trajectory of becoming an internal practitioner of the pelvic floor.
I have designed the Athletes and Pelvic Rehabilitation course to reach both the sports and orthopedic clinician as well as the pelvic health practitioner who might be a veteran of pelvic floor education and treatment. Both groups will leave this course with additional tools for their clinical tool box in the realms of manual therapy and exercise.2 Here are some of the objectives for the course:
- Provide clinicians that do not perform internal work a better and more complete understanding of how the pelvic floor integrates into human movement, particularly higher-level activities such as running, lifting and all types of sporting movements.
- Provide both the experienced and pelvic floor early learner with a comprehensive paradigm of exercise theory, development and progressions as well as how to provide non-internal manual therapy to influence the performance of the pelvic floor.
- Provide strategies for clinicians to determine when your patient would be better served with a referral to a pelvic health practitioner and what the current evidence is to support your decision.
- Create innovative and engaging therapeutic exercise programs (home exercise programs too!) for your patients directed at the pelvis with specific attention to upright and functional positioning.
What do people who have attended courses with Dr. Dischiavi have to say? Janna wrote the following email to Herman & Wallace about Steve's Course:
"Good morning. I wanted to make sure that you knew what a fantastic clinician you have to join your team in Steve Dischiavi. I am a practicing OB and orthopedic therapist and felt this course was fantastic! Usually the main goal is to come away with a couple of clinical "pearls." I felt as though I came away with a full days worth of "pearls." I really liked that the course was not totally pelvic floor based, however was totally relevant to the women's health population, but it will also apply to the majority of my current patient population as well. Thank you for the opportunity to learn from Steve!"
1. Orchard JW. Men at higher risk of groin injuries in elite team sports: a systematic review. Br J Sports Med. 2015;49(12):798-802.
2. Tuttle L. The Role of the Obturator Internus Muscle in Pelvic Floor Function. Journal of Women’s Health Physical Therapy. 2016;40(1):15-19.
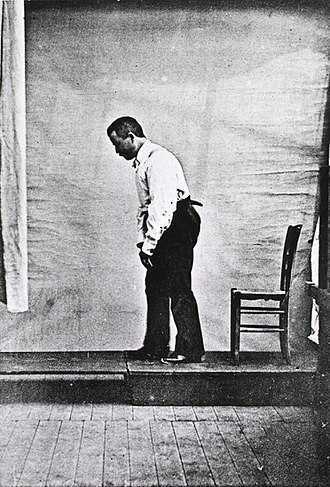
Akinesia is a term typically used to describe the movement dysfunction observed in people with Parkinson disease. It is defined as a poverty of movement, an impairment or loss of the power to move, and a slowness in movement initiation. There is an observable loss of facial expression, loss of associated nonverbal communicative movements, loss of arm swing with gait, and overall small amplitude movements throughout all skeletal muscles in the body. The cause of this characteristic profile of movement is due to loss of dopamine production in the brain which causes a lack of cortical stimulation for movement.
 If the loss of dopamine production in the brain causes this poverty of movement in all skeletal muscles the body, how does the pelvic floor function in the person with Parkinson disease and what should the pelvic floor rehabilitation professional know about treating the pelvic floor in this population of patients?
If the loss of dopamine production in the brain causes this poverty of movement in all skeletal muscles the body, how does the pelvic floor function in the person with Parkinson disease and what should the pelvic floor rehabilitation professional know about treating the pelvic floor in this population of patients?
Let’s take a closer look referencing a very telling article about Parkinson disease and skeletal muscle function. In the Italian town of L’Aquila, a major devastating 6-point Richter scale earthquake occurred on April 6, 2009. 309 people died and there was destruction and collapse of many historical structures, some greater than 100 years old. The nearby movement disorder clinic had been following 31 Parkinson disease patients in the area, 17 of them higher functioning and the other 14 much lower functioning. In fact, of those 14, 10 of them were affected by severe freezing episodes with severe nighttime akinesia requiring assistance with bed mobility tasks, 1 was completely bedridden and the others with major fluctuations in motor performance. 13 of the 14 patients also had fluctuating cognitive functioning.
This devastating earthquake occurred at 3:30 am. All 14 of these patients were able to escape from their homes during or immediately following the event. Caregivers reported that in the majority of the cases, the person with Parkinson’s disease was the first one to be alerted to the earthquake, the first one to get out of the house, ability to alert relatives to run for safety, physically assisting relatives out of the collapsing buildings, and in some cases independently escaping down 1-2 flights of stairs.
Paradoxical kinesia is thought to be the reason for this all but sudden ability to move normally within the presence of an immediate threat to their life and lives of loved ones. Paradoxical kinesia is defined as “a sudden and brief period of mobility typically seen in response to emotional and physical stress in patient’s with advanced idiopathic Parkinson’s disease.” There are a few mechanisms hypothesized to play a role, such as, adrenaline, dopaminergic reserves activating the flight reaction, and compensatory nearby cerebellar circuitry.
There is no pathological evidence that in Parkinson disease there is any break in the continuity of the motor system. The neurologic pathways are all intact and the ability to produce muscle power is retained however requires a strong base of clinic knowledge of the disease to help these patients activate these intact motor pathways. I look forward to sharing the neurologic basis of these deficits in Parkinson disease and strategies in pelvic floor rehab to do just that!
Erica Vitek, a specialist in treating patients with neurologic dysfunction, is the author and instructor of Neurologic Conditions and Pelvic Floor Rehab, taking place September 14-16, 2018 in Grand Rapids, MI.
Bonanni, L., Thomas, A., Anzellotti, F., Monaco, D., Ciccocioppo, F., Varanese, S., Bifolchetti, S., D’Amico, M.C., Di Iorio, A. & Onofrj, M. (2010). Protracted benefit from paradoxical kinesia in typical and atypical parkinsonisms. Neurological sciences, 31(6), 751-756.
The following is a guest submission from Alysson Striner, PT, DPT, PRPC. Dr. Striner became a Certified Pelvic Rehabilitation Practitioner (PRPC) in May of 2018. She specializes in pelvic rehabilitation, general outpatient orthopedics, and aquatics and treats at Carondelet St Joesph’s Hospital in the Speciality Rehab Clinic located in Tucson, Arizona.
Recently, I had a patient present with Complex Regional Pain Syndrome (CRPS) on his right foot. He stated that the pain had started about 10 days after his prostatectomy when someone had fallen onto his right foot. He reported a bunionectomy on that foot 7 years prior and noted an episode of plantar facilities before his prostatectomy. CRPS is defined as “chronic neurologic condition involving the limbs characterized by severe pain along with sensory, autonomic, motor, and trophic impairments” in a 2017 article "Complex regional pain syndrome; a recent update" by Goh, En Lin. The article goes on to discuss how CRPS can set off a cascade of problems including altered cutaneous innervation, central and peripheral sensitization, altered sympathetic nervous system function, circulating catecholamines, changes in autoimmunity, and neuroplasticity.
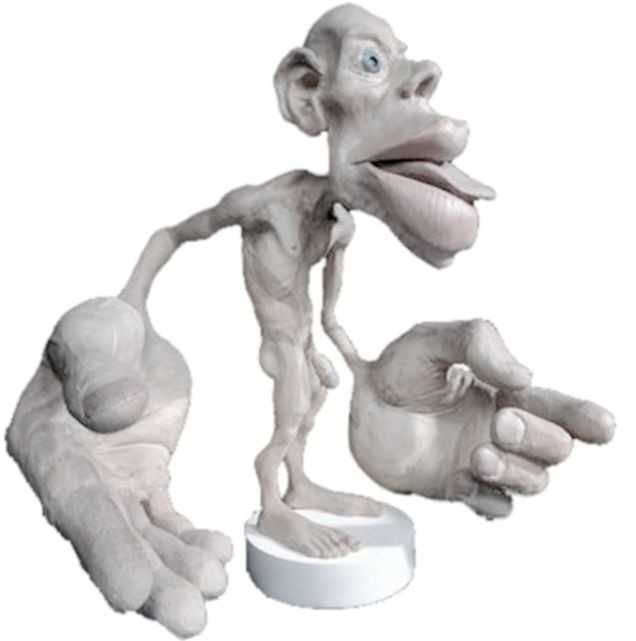
 A recent persistent pain theory to explain the relationship between pelvic floor and his foot could be overflow or ‘smudging’ in his homunculus. The homunculus is the map of our physical body in our brain where the feet are located next to the genitals. Possibly when one has pain, there can be ‘smudging’ of our mental body map from one area into another. I have heard this explained as though a chalk or charcoal drawing has been swipes their hand through the picture. A recent study by Schrabrun, SM et al “Smudging of the Motor Cortex is Related to the Severity of Low Back Pain” found that people with chronic low back pain had a loss of cortical organization which and that this loss was associated with the severity and location of LBP.
A recent persistent pain theory to explain the relationship between pelvic floor and his foot could be overflow or ‘smudging’ in his homunculus. The homunculus is the map of our physical body in our brain where the feet are located next to the genitals. Possibly when one has pain, there can be ‘smudging’ of our mental body map from one area into another. I have heard this explained as though a chalk or charcoal drawing has been swipes their hand through the picture. A recent study by Schrabrun, SM et al “Smudging of the Motor Cortex is Related to the Severity of Low Back Pain” found that people with chronic low back pain had a loss of cortical organization which and that this loss was associated with the severity and location of LBP.
There are many ways to improve the organization of the homunculus and create neuroplasticity. One such way was suggested is with Transcutaneous electrical nerve stimulation (TENS) to the bottom of the foot to affect bladder spasms and pain. In recent study, “Transcutaneous electrical stimulation of somatic afferent nerves of the foot relieved symptoms related to postoperative bladder spasms,". Zhang, C et al. 2017 found that participates that had either a bladder surgery or a prostate surgery had improvement in bladder spasm symptoms and VAS scores on day two and three. Their protocol was to use two electrodes over the bottom of the foot at 5 Hz with 0.2 millisecond pulse width until a muscle twitch was achieved and was increased, but still comfortable for an hour (there is a picture of electrode placement in the article). The authors note that this neuromodulation of the foot sensory nerves may inhibit interactions between the somatic peripheral neuropathway and autonomic micturition reflex to calm the bladder and pain.
No matter what we do to help calm nervous systems from the top down; pain neuroscience education, mindful based relaxation, graded motor imagery, or from the bottom up; de-sensitization, biofeedback, or good old-fashioned TENS. The result is the same; a cortical organization and happier patients.
En Lin Goh†, Swathikan Chidambaram† and Daqing Ma. "Complex regional pain syndrome: a recent update". Burns & Trauma 2017 5:2.https://doi.org/10.1186/s41038-016-0066-4"
Schabrun SM, Elgueta-Cancino EL, Hodges PW. "Smudging of the Motor Cortex Is Related to the Severity of Low Back Pain." Spine (Phila Pa 1976). 2017 Aug 1;42(15):1172-1178. doi: 10.1097/BRS.0000000000000938
Chanjuan Zhang, et al. "Transcutaneous electrical stimulation of somatic afferent nerves in the foot relieved symptoms related to postoperative bladder spasms". BMC Urol. 2017; 17: 58. doi: 10.1186/s12894-017-0248-9
All Upcoming Continuing Education Courses

Pelvic Function Level 1 - Satellite - Milwaukee WI - July 12 - 13 2025 - SOLD OUT
Jul 12 2025 - Jul 13 2025

Modalities and Pelvic Function - In-Person - Houston TX - July 12 - 13 2025
Jul 12 2025 - Jul 13 2025

Pelvic Function Level 1 - Satellite - Denver CO - July 12 - 13 2025 - SOLD OUT
Jul 12 2025 - Jul 13 2025




Pelvic Function Level 1 - Satellite - Des Moines IA - July 26 - 27 2025 - SOLD OUT
Jul 26 2025 - Jul 27 2025

Pelvic Function Level 1 - Satellite - Minneapolis MN - July 26 - 27 2025 - SOLD OUT
Jul 26 2025 - Jul 27 2025

Pelvic Function Level 1 - Satellite - Paso Robles CA - July 26 - 27 2025 - SOLD OUT
Jul 26 2025 - Jul 27 2025

Pelvic Function Level 1 - Satellite - St. Augustine FL - July 26 - 27 2025
Jul 26 2025 - Jul 27 2025

Pelvic Function Level 1 - Satellite - Virginia Beach VA - July 26 - 27 2025 - SOLD OUT
Jul 26 2025 - Jul 27 2025


Pelvic Function Level 1 - In-Person - Chicago IL - August 2 - 3 2025 - SOLD OUT
Aug 2 2025 - Aug 3 2025



Menopause Transitions and Pelvic Rehab - Remote Course - August 9 - 10 2025
Aug 9 2025 - Aug 10 2025









Pelvic Function Level 2C - Satellite - Palm Beach FL - August 16 - 17 2025
Aug 16 2025 - Aug 17 2025

Pelvic Function Level 2C - Satellite - New Orleans LA - August 16 - 17 2025
Aug 16 2025 - Aug 17 2025
Pelvic Function Level 2C - Satellite - Paso Robles CA - August 16 - 17 2025
Aug 16 2025 - Aug 17 2025


Pediatrics Level 1 - Treatment of Bowel and Bladder Disorders - Remote Course - August 23 - 24 2025
Aug 23 2025 - Aug 24 2025

Pelvic Function Level 1 - Satellite - Jacksonville FL - August 23 - 24 2025
Aug 23 2025 - Aug 24 2025

Pelvic Function Level 1 - Satellite - Chicago IL - August 23 - 24 2025 - SOLD OUT
Aug 23 2025 - Aug 24 2025


Rehabilitative Ultrasound Imaging Pelvic Health Satellite Lab Course - Self-Hosted - September 5 - 7 2025
Sep 5 2025 - Sep 7 2025
Rehabilitative Ultrasound: Orthopedic Topics Satellite Lab Course - Self-Hosted - September 5 - 6 2025
Sep 5 2025 - Sep 6 2025

Rehabilitative Ultrasound Imaging Pelvic Health Satellite Lab Course - Indianapolis IN - September 5 - 7 2025
Sep 5 2025 - Sep 7 2025
Rehabilitative Ultrasound: Orthopedic Topics Satellite Lab Course - Indianapolis IN - September 5 - 6 2025
Sep 5 2025 - Sep 6 2025
