
The popularity of yoga continues to rise with over 36 million yogis living in the United States of America and over 300 million practitioners worldwide. Yoga has several therapeutic effects that make it a beneficial addition to home exercise programs for practitioners and personal practice.
Dustienne Miller discussed some of the benefits of yoga in her March blog (March 8, 2022 - A yoga practice can change your neuroanatomy!). These benefits extend beyond the musculoskeletal system and include improved mood and depression, changes in pain perception, improved mindfulness and associated improved pain tolerance, and the ability to observe situations with emotional detachment.
The physical benefits are well documented in several research studies and include improved flexibility, strength, and stability as well as enhanced respiratory and cardiovascular function. Supporting documentation also shows that yoga can help alleviate the symptoms of chronic pain. Dustienne Miller shared that in a study by Villemure et al, they determined “that the insula-related interoceptive awareness strategies of the yoga practitioners being used during the experiment correlated with the greater intra-insular connectivity...concluding that the insular cortex can act as a pain mediator for yoga practitioners.”
Restorative yoga shares the many benefits seen in other styles of yoga and can also be a great addition to home programs for pelvic rehab practitioners. Kate Bailey shared in her interview with The Pelvic Rehab Report (August 31, 2021 – Faculty Interview: Kate Bailey) that restorative yoga “focuses on the lesser-known aspects of the yoga platform: breath, restorative practice, and a bit of meditation. I have clients all the time who struggle with meditation because their nervous systems aren’t ready for it. So we look at breathing and restorative yoga both as independent alternatives, but also as a way to get closer to meditation.. giving the clinicians another skill for their own rest practice can be useful when feeling tired, overwhelmed, or burned out. “
But what does this mean? Let’s look at some of these aspects a bit closer:
Improving mood and sleep: This includes depression, anxiety, and even stress or other mood disorders. Consistent yoga practice can lead to significant increases in serotonin levels coupled with decreases in the levels of monoamine oxidase, an enzyme that breaks down neurotransmitters and cortisol(1). Yoga can inhibit the areas in the brain responsible for fear, aggressiveness, and rage (posterior or sympathetic area of the hypothalamus) – while simultaneously stimulating the rewarding pleasure centers in the median forebrain and other areas leading to a state of bliss and pleasure. This inhibition results in lower anxiety, heart rate, respiratory rate, blood pressure, and cardiac output (2).
Think about it. Deep breathing calms the nervous system. This promotes relaxation. The more relaxed you are then the better the chance of having a good night’s sleep. Consistent yoga practice can also assist sleep quality by increasing melatonin and reducing hyperarousal (3). Pratyahara, or a turning inward of the senses, allows downtime for the nervous system and can be encouraged by yoga poses such as savasana (corpse pose) and pranayama (breathing exercises/control.
Reduced Chronic Pain: Asana and meditation have been shown to reduce chronic pain including reduced pain from arthritis, back pain, and other chronic conditions while also improving balance and increasing proprioception(1). Yoga sessions can take our joints through a full range of motion. This squeezes and soaks areas of cartilage not often used and provides fresh nutrients, oxygen, and blook to the joints. Otherwise neglected areas of cartilage in the joints would wear out, exposing bone, which can lead to arthritis and chronic pain. At the same time, yoga is gentle on the body and consistent practice can strengthen the connective tissues that surround the bones and joints.
Effects on Cancer Patients: Yoga cannot cure cancer, but it can reduce stress and improve physical, emotional, and spiritual wellness. There is supporting research that the growth of cancerous tumors can be exacerbated by stress(4). This same study found that consistent yoga practice could decrease post-chemotherapy-induced frequency and intensity of nausea and the intensity of anticipatory nausea and vomiting. In 2018 Lin et al provided new research showing that restorative yoga can decrease depression in cancer survivors; improve symptoms of anxiety, depression, and pain symptoms in cancer patients; and help patients manage the toxicity of cancer treatments (5). In addition, yoga has a fundamental emphasis placed on mindfulness and acceptance of your body and its limitations.
Kate Bailey likes to joke about lying on the floor, but really, it is not a joke at all. Lying on the floor for 15 minutes is savasana. She shares that “Savasana is a wakeful resting and a practice of relaxation response. It seems easy: you always have access to a floor. You don’t need anything fancy. Aside from the neuroregulatory benefits of rest, savasana also gives the postural muscles a break. It allows the hip flexors to re-lengthen and the cervicothoracic junction to realign.”
Let’s take a moment to close with a savasana (did you know that a 5-minute savasana is recommended for every 30 minutes of yoga?). This pose can calm the central nervous system, aid the digestive and immune systems, reduce headaches, fatigue, and anxiety while lowering blood pressure and calming the mind, and reducing stress.
Take a moment and lay on the floor with your arms and legs open wide and relaxed (starfish style), supported by a bolster, or you may want to place your hands gently over your chest or your stomach. Now gently still your body. Release your breath and be present. Be completely aware of the moment. Let your mind and body go for a few moments.
Namaste.
References:
- McCall T. New York: Bantam Dell a division of Random House Inc; 2007. Yoga as Medicine.
- Woodyard C. Exploring the therapeutic effects of yoga and its ability to increase quality of life. International journal of yoga, 4(2), 49–54. 2011. doi: 10.4103/0973-6131.85485
- Wang W-L, Chen K-H, Pan Y-C, Yang S-N, Chan Y-Y. The effect of yoga on sleep quality and insomnia in women with sleep problems: A systematic review and meta-analysis. BMC Psychiatry. 2020;20(1):195. doi:10.1186/s12888-020-02566-4
- Carson, J. W., Carson, K. M., Porter, L. S., Keefe, F. J., Shaw, H., & Miller, J. M. (2007). Yoga for women with metastatic breast cancer: results from a pilot study. Journal of pain and symptom management, 33(3), 331–341.
- Lin P-J, Peppone LJ, Janelsins MC, et al. Yoga for the management of cancer treatment-related toxicities. Curr Oncol Rep. 2018;20:5. doi:10.1007/s11912-018-0657-2
 Restorative Yoga for Physical Therapists with instructor Kate Bailey
Restorative Yoga for Physical Therapists with instructor Kate Bailey
This course will provide the basis for experiencing and integrating restorative yoga into physical therapy practice. Restorative yoga is an accessible practice that can teach patients (and practitioners) how to rest systematically, for short periods of time, on a regular basis to encourage the parasympathetic nervous system to balance with the sympathetic nervous system for improved neuroregulation. Topics include the difference between meditation and restorative yoga, and how they can support each other in order to support the ability to drop into relaxation. Restorative postures, each taking 20-30 minutes are offered prior to the live meeting so that participants can experience what a patient might experience when restorative yoga is a component of their home program. Then in the live course participant experiences, questions, and strategies on how to reduce barriers to relaxation so that patients can integrate this practice into their lifestyle will be discussed. There will also be live labs for breathing techniques and specific meditations that may be helpful to patients working with an unregulated nervous system.
 Yoga for Pelvic Pain with instructor Dustienne Miller
Yoga for Pelvic Pain with instructor Dustienne Miller
This course offers an evidence-based perspective on the value of yoga for patients with chronic pelvic pain by focusing on two of the eight limbs of Patanjali’s eightfold path: pranayama (breathing) and asana (postures) - and how they can be applied for patients who have hip, back and pelvic pain. A variety of pelvic conditions will be discussed including interstitial cystitis/painful bladder syndrome, vulvar pain, coccydynia, hip pain, and pudendal neuralgia. Lecture topics include the role of yoga within the medical model, contraindicated postures, and how to incorporate yoga home programs as therapeutic exercise and neuromuscular re-education both between visits and after discharge.


This article was originally posted on the Medbridge Blog site: https://www.medbridgeeducation.com/blog/2021/11/six-actionable-ways-to-be-a-better-lgbtq-ally/.
Brianna Durand, PT, DPT earned her Doctor of Physical Therapy at Texas Woman’s University in Houston, TX. During graduate school, she led and co-founded PT Proud, a Catalyst Group within the Health Policy and Administration Section of the APTA, to improve the education, equity, and inclusion of LGBTQ+ patients, students, and clinicians. Brianna owns and operates Empower Physiotherapy, a private practice in Seattle. As a competitive powerlifter, Brianna enjoys working with strength athletes who experience pelvic floor dysfunction, especially stress incontinence. She is passionate about providing care to individuals in the LGBTQ+ community, including those undergoing hormonal/surgical transition. Brianna's additional clinical interests include prenatal/postpartum care for trans and gender-nonconforming folx and pelvic floor care for patients that are intersex. Brianna curated and teaches LGBTQ+ cultural competency for practitioners in her course - Inclusive Care for Gender and Sexual Minorities.
LGBTQIA2S+. Does it seem like that acronym is ever-growing? That’s because it is!
As our society evolves, more people are feeling safe and comfortable to live as their authentic selves, and every day there is more evidence to support that.
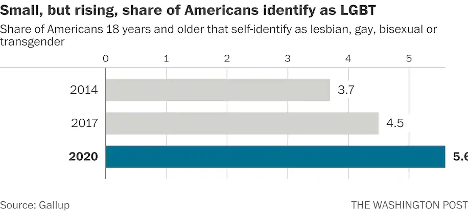
According to Gallup polls, the percentage of people in the U.S. that identify as lesbian, gay, bisexual, or transgender has increased to 5.6 percent.3 That is three times the entire population of Colorado! These numbers are even higher amongst younger generations—up to 20 percent in Gen Z and millennials by some estimates. In 2019, nearly 80 percent of surveyed Americans state that they personally know someone who identifies as LGBTQIA2S+ or queer.2 And while the word “queer” has a nasty history as a derogatory slur, it is increasingly used by folks in the LGBTQIA2S+ community to describe those who do not identify as cisgender or heterosexual.
What Is the Importance of Sexual Orientation or Gender Identity in Healthcare?
Recent years have provided a groundswell of awareness building around this community—from representation in entertainment, discussion about participation in athletics, and changes occurring at the legislative level. However, one area of society in which awareness is still lacking is in modern-day medicine, so let’s explore the significance of sexual orientation and gender identity (SOGI) as it pertains to healthcare.
As a medical professional, you may wonder “Can’t I simply treat all people the same?” While this idea may be filled with good intentions, the unfortunate reality is that we do not yet have access to this utopian future. There are real, measurable differences in the health of all marginalized communities, including gender and sexual minorities (GSM).
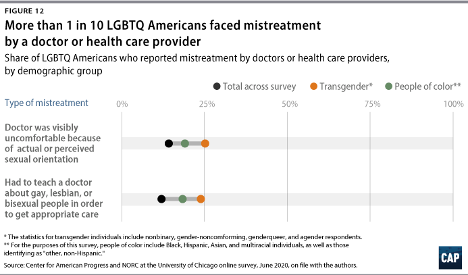
In 2020, 1 in 10 LGBTQIA2S+ Americans faced some form of mistreatment from a healthcare professional.1 These negative experiences strongly correlate with postponing or altogether avoiding medical care in the future, further contributing to the collective LGBTQIA2S+ fear of discrimination. The statistics are even worse when specifically looking at queer and trans people of color.
What Can You Do as a Healthcare Provider?
While the system and the education that trains our clinicians could benefit from a renovation, here are six actionable steps you can take now to facilitate a safer space for your LGBTQIA2S+ patients:
1. Recognize your own potential to cause harm.
As healthcare professionals, we have some degree of inherent privilege. With this privilege comes the capacity to inflict harm, intentional or not. While intentions matter, they do not supersede the impact your words or actions have on another. Assumptions matter, too. While assumption making is common and normal—an evolutionarily advantageous adaptation of the brain—they are not facts, and they are not harmless. Erroneous assumptions about a person’s gender or sexual identity by a medical professional can lead to behaviors that cause discomfort in and discrimination towards LGBTQIA2S+ patients and clients, even if inadvertently.
By recognizing the power differential that exists in the patient/provider relationship and the implications that come with it, we are likely to be more aware of our words and actions when they come up, and more willing to address them when they do. And by taking a position of genuine care and curiosity rather than assumption, we can affirm the relationship between the person whom we are helping and their body.
2. Update your language.
Always use the correct pronouns and name of the person with whom you are working. One easy way to do this is simply by mirroring the language they use when describing themself. However, if you are meeting someone for the first time, you may unintentionally use language that is not in line with your patient or client’s identity. For example, you may use someone’s dead name (the name assigned to them at birth) which may still be listed on their legal and medical documentation.
You can preempt this kind of unintentional harm by including areas for clarification on intake paperwork. This will allow you the opportunity to affirm the pronouns of the person in your care upon your first interaction. While pronoun affirmation may seem like a small action, it has shown to be effective in reducing suicidal ideation and depression.4 Another way to update your language for greater inclusivity is by using the term “spouse” or “partner” when inquiring if a patient has someone at home that can help with their activities of daily living or rehabilitation. Additionally, when referring to pregnancy, birthing, and postpartum care, practice saying “pregnant person” or “birthing parent” rather than “pregnant woman” or “mother.”
3. Speak up….even if the LGBTQIA2S+ person or target of the harm isn’t present.
Shaming someone’s behavior is unlikely to result in positive change or self-reflection. Instead, we can follow the steps of stopping, educating, and being proactive to foster learning in our colleagues. This kind of dialogue offers the opportunity for the individual to participate in the discussion by learning about their behavior, rather than feeling pushed out of the conversation which could limit their chance to grow.
- First, STOP the discussion or action taking place by intervening with “Those words can be hurtful.”
- Next, EDUCATE in lieu of asserting judgment. Proceed from a lens of curiosity. Asking the person “Do you know what those words mean?” or genuinely inquiring about their intention and understanding. Doing this will facilitate conversation and enhance one’s knowledge of their damaging actions, reducing the chance that they will repeat the harmful behavior.
- Finally, BE PROACTIVE by following up with resources for further learning such as GLMA, WPATH, or The Fenway Institute.
It is important to note the significance of taking this action even if the LGBTQIA2S+ person was not present for the encounter. This breaks the notion that harmful language is acceptable so long as the subject of the harm is not privy to it. If the LGBTQIA2S+ person is present for the encounter, it is best to first pull them aside to check in with them, make sure they are alright, and ask if they want your help. Some folks prefer to avoid drawing attention to themselves. It is also a skill of allyship to know when not to talk.
4. Be receptive to feedback.
When an LGBTQIA2S+ person, or a person from any marginalized group for that matter, corrects your language or behavior, practice saying “thank you” rather than “sorry” and avoid explaining yourself. It is a privilege to learn about oppression rather than to experience it for yourself. When someone corrects you, not only are they bravely honoring their authentic identities, but they are doing emotional labor on your behalf, and in the age of freely available information, it is never the responsibility of marginalized folks to educate others for free. These interactions are opportunities for personal growth—don’t let them pass you by!
5. Suggest practical changes to make the workplace more inclusive.
Does your workplace have gender-neutral bathrooms? Many LGBTQIA2S+, queer, and trans people avoid using public restrooms to avoid harassment and violence. Such aggressions can have very tangible consequences to their physical health, such as pelvic floor dysfunction. If there aren’t any inclusive restrooms in your workplace, make a suggestion to change that.
How inclusive are the brochures in your waiting room? Do the patient education materials that you provide to a patient after evaluation use language and imagery that include the LGBTQIA2S+ community? These are areas that can be improved upon with the suggested language updates we discussed above in action step two.
Are there symbols or graphics that will welcome GSM, such as safe space signs, flags depicting an upside-down rainbow triangle, or “all-gender” verbiage in lieu of gender-specific? Both would make easy additions that signal to patients they are in an inclusive space. However, it is important to distinguish the difference between saying a space is safe, and actually making a space safe. A space can only be safe if the entire team of providers and office staff are on board. Labeling a space as safe when it is not has the propensity to cause further harm. Be sure before these indicators are put up in your practice, everyone is ready to support such efforts.
6. Be prepared to mess up—but don’t let that deter you from trying.
Any etymologist will tell you that languages are living things that are constantly evolving. Developments such as these can make it challenging to stay current on which terminology is most beneficial to our growing society. Sometimes just the fear of making a mistake can be intimidating enough to discourage people from trying. What is most important is not how well you use updated language but that you are trying. Your effort matters, and it is what will move the needle in the right direction. Cultural responsiveness is not knowing every nuanced detail of every demographic group. Cultural responsiveness is being willing to reflect and modify your viewpoints when presented with information that differs from what you previously held to be true. Try to accept that just with learning any new skill, mistakes are bound to happen. When they do be prepared to learn, and then move forward with that new knowledge in mind.
References:
- Cusick Director, J., Seeberger Director, C., Woodcome, T., Oduyeru Manager, L., Gordon Director, P., Shepherd, M., Parshall, J., Santos, T., Medina, C., Gruberg, S., Mahowald, L., Bleiweis, R., Graves-Fitzsimmons, G., & Zhavoronkova, M. (2021, November 7). The State of the LGBTQ Community in 2020. Center for American Progress. Retrieved November 23, 2021, from https://www.americanprogress.org/article/state-lgbtq-community-2020/.
- Ellis, S. K. (2019). GLAAD Accelerating Acceptance 2019 Executive Summary. GLAAD.
- Jones, J. M. (2021, November 20). LGBT identification rises to 5.6% in latest U.S. estimate. Gallup.com. Retrieved November 23, 2021, from https://news.gallup.com/poll/329708/lgbt-identification-rises-latest-estimate.aspx.
- Russell, S. T., Pollitt, A. M., Li, G., & Grossman, A. H. (2018). Chosen name use is linked to reduced depressive symptoms, suicidal ideation, and suicidal behavior among transgender youth. Journal of Adolescent Health, 63(4), 503–505. https://doi.org/10.1016/j.jadohealth.2018.02.003
Additional resources:
- Schmidt, S. (2021, February 26). 1 in 6 Gen Z adults are LGBT. and this number could continue to grow. The Washington Post. Retrieved November 23, 2021, from https://www.washingtonpost.com/dc-md-va/2021/02/24/gen-z-lgbt/.
- Who Are We? Consortium. (n.d.). Retrieved November 23, 2021, from https://www.consortium.lgbt/intersex-inclusive-flag/.
Inclusive Care for Gender and Sexual Minorities
with instructor Brianna Durand, PT, DPT
When it feels overwhelming and nuanced, it can be tempting to avoid uncomfortable topics altogether. However, attendees for this course can expect to be gently guided into the sometimes confusing realm of gender and sexual orientation, and identity. This course will provide a safe space to ask all the questions about caring for LGBTQ+ patients and practicing the skills needed to help advance your practice. Although this course will cover pelvic floor physical therapy specifically, it is appropriate and useful for any medical professional as we all have patients in the LGBTQ+ community.

This week The Pelvic Rehab Report sat down with new faculty member, Emily McElrath PT, DPT, MTC, CIDN, to discuss her pelvic rehab journey and her new course, Pregnancy and Postpartum Considerations for High-Intensity Athletics. Emily is a native of New Orleans, is highly trained in Sports and Orthopedics, and has a passion for helping women achieve optimal sports performance. Emily is also certified in manual therapy and dry needling, which allows her to provide a wide range of treatment skills including joint and soft tissue mobilization. She is an avid runner and Crossfitter and has personal experience modifying these activities during pregnancy and postpartum.

Hi Emily! Can you tell us a little bit about yourself and your clinical practice?
My name is Emily McElrath, and I am an orthopedic and pelvic floor PT. I spent the early years of my career in sports medicine and primarily worked with high school and collegiate athletes, as well as weekend warriors. I myself am a distance runner and Crossfitter and have always had a love for sports. After the birth of my second child, I had a hard time returning to Crossfit due to significant pelvic floor dysfunction and pain. At that time, I became a pelvic floor patient and quickly realized how valuable this specialty was. This began my journey to becoming a pelvic PT.
Since that time almost 4 years ago, I have been blending my orthopedic and pelvic health knowledge and skillset to help women return to the sports they love without pain and pelvic floor dysfunction. My main goal as a clinician is to educate and empower my patients to feel in control of their own bodies, and to feel confident in daily and recreational activities.
What has your educational journey as a pelvic rehab therapist looked like and how did you get involved in the pelvic rehabilitation field?
It was really a matter of personal experience leading me to the field of pelvic health. I knew the specialty of pelvic health existed, but until I was a patient I did not truly appreciate how valuable it was. Seeing firsthand how significantly pelvic floor physical therapy could improve the quality of a patient’s life gave me a desire to become a pelvic PT. Once I got into my course work with Herman & Wallace, I realized that my background as an orthopedic PT would blend well with pelvic PT. It also gave me a lot of perspective into how significant of a role the pelvic floor plays in the entire kinetic chain. I would even say that my pelvic floor education has helped me be a more thorough orthopedic clinician. It has helped me think outside the box and enabled me to be more thorough in my critical thinking when evaluating patients.
What patient population do you find most rewarding in treating and why?
I have two patient populations that I find most rewarding. The first is HIIT athletes. I find this population so fun to work with. They are some of the most dedicated and compliant patients I have. Their love of their sport is often a driving force for them to get and stay healthy. Many of these athletes will even come to my clinic without having pain or dysfunction. They are strictly coming for education and prevention, which I love. After all, PTs as a profession are huge proponents of wellness and prevention. I also love teaching a patient that they can, in fact, continue doing exercises they may have been previously told were not safe to do during pregnancy or postpartum. Giving them hope that they can continue doing what they love after they were afraid they may not is very rewarding.
The second population I love working with is my childbirth prep patients. I LOVE education. I feel like these sessions really highlight that part of physical therapy. These sessions not only address any current concerns a patient is having but also provide education to give them the confidence to birth the way they want. I review everything from what to expect during labor, to different positions for pushing, and how to push. I even have partners come to the sessions so they can learn how to best support the patient during delivery. Hearing from patients that their birth experience was beautiful and just as they had hoped always gives me a lot of joy. I feel honored to be able to be a part of that journey.
What do you find is the most useful resource for your practice?
I find other practitioners the most valuable resource in my practice. There is so much that can be gained from collaborating with other pelvic PTs, doulas, midwives, OB/GYN, sex therapists, etc. Pelvic rehab is so multifaceted, that I believe it truly requires a collaborative approach to provide the best patient outcomes.
What books or articles have impacted you as a clinician?
There was a recent article that came out about the prevalence and significance of Levator Ani avulsion tears. This was an interesting article because I have seen this more and more clinically, but there is very little research on the matter. My favorite books as a clinician are: “The Body Keeps the Score”, “Come As You Are”, and “Pelvic Pain Explained”.
What lesson have you learned in a course, from an instructor, or from a colleague or mentor that has stayed with you?
I think the biggest thing I have learned is that the objective findings of our evaluations are only a small part of the puzzle. Pelvic rehab is an intimate type of physical therapy, and many of our patients may have had trauma that is still raw to them. If most of your evaluation is spent talking with the patients to ensure they feel comfortable, that’s ok. I have realized that it’s ok if I don’t get to every objective test and measure in the first session. In this line of work, patient comfort is most important. Building a rapport with your patient must take precedent.

What made you want to create this course, Pregnancy and Postpartum Considerations for High-Intensity Athletics?
I wanted to create this course because I saw a need in the Crossfit community for more education on how to safely train pregnant and postpartum athletes, and I feel physical therapy is a great place to start, after all, PTs are experts in the musculoskeletal system. We are seeing more and more of these HIIT athletes becoming moms and wanting to maintain their athleticism throughout pregnancy & postpartum, and I think that’s great!
With that being said, I think there are nuances to training this athletic population. There are so many hormonal, anatomical, and structural changes to consider during pregnancy & postpartum, and that may affect how well an athlete can tolerate strain. However, most of these changes are not contraindications to training. Therefore, we as rehab practitioners and physical therapists need to fully understand the demands of HIIT, as well as the specific considerations for this population so that we can keep them safely and effectively doing what they love.
What need does your course fill in the field of pelvic rehabilitation?
By and large, people do not fully understand the demands of HIIT activities like Crossfit unless they personally partake in these activities. This includes healthcare professionals like physical therapists. However, many of our pregnant and postpartum athletes will require the care of a PT (especially pelvic) at some point throughout their pregnancy, and postpartum journey.
My course, Pregnancy and Postpartum Considerations for High-Intensity Athletics bridges the gap between education and experience, for those healthcare professionals who do not personally participate in HIIT to understand the demands of the sport. It also helps those physical therapists who do not specialize in pelvic health to understand the unique demands of this athlete population from a pelvic health perspective.
Who, what demographic, would benefit from your course?
Any PT, PTA, PT student, OT, COTA, or OT student who is looking to better understand the demands of HIIT, the special considerations for pregnant and postpartum athletes who participate in HIIT, and how to safely train and treat these athletes to help them continue to do what they love.
If you could get a message out to physical therapists about pelvic rehab what would it be?
Oh man, where do I start? There are so many things I want to shout from the mountain tops about pelvic PT. It truly is a gem in the field of physical therapy, and I think is often a missing link in traditional physical therapy care. Pelvic rehab is so much more than urinary leakage and kegels. It can be so impactful to the quality of life of a patient. There is no other area of the body that is critical to so many functions but is also so vastly overlooked and undertreated. The need for research, education, and development in this field is critical if we are going to have a true “whole body” approach to treatment.
Join H&W and Emily McElrath on May 21st to learn more about this patient demographic in Pregnancy and Postpartum Considerations for High-Intensity Athletics

Hi Kate, can you tell us about the course you have designed Restorative Yoga for Physical Therapists?
My name is Kate Bailey and I am a pelvic floor physical therapist. I’ve been a pelvic floor PT going on4-5 years now. Before that, I’ve been a pilates instructor for 20 years and taught yoga for over a decade. This course is a culmination of all of my experiences both with the yoga, pilates, and the pelvic floor population from kiddos through adulthood. It allows us to use the techniques from the yoga and pilates philosophies to support people in their healing process from pelvic pain and also just in their bodies.
What can participants expect to learn when they come to the course?
I wrote this course when the pandemic started. My whole intention was to make the didactic information self-paced and watch the videos as often as you want kind of course. This way, when we have dedicated time together it’s a lot more about discussion and me guiding people through the labs, and in turn, they can guide their colleagues or patients. It is designed so I’m not spending a lot of time lecturing to a screen and our time dedicated to each other is more about a conversation. I want people to learn about the information in their own time, marinate in it a little bit, and then come with questions.
How do you feel that restorative yoga fits in with the care we provide to our patients with pelvic health conditions?
The restorative yoga component to me is really special because it’s one of the only times we prioritize rest, and not doing, and sitting with ourselves. Not necessarily trying to get strong, or trying to get more flexible. It’s really about allowing our bodies to be. Sometimes that is being in a little bit of discomfort. Sometimes that is just being with the exhaustion that I think we all have a little bit of. Just learning how to be with ourselves for 8, to 12, to 15 minutes and see that as a really productive part of our treatment plan.
How does trauma-informed care influence your course?
One of the things that I highlight in the course is how much trauma occurs in and around the home. So when we’re asking patients to do a home program one of the discussion points we have in the course is “what if the home is inherently triggering or unsafe?” How can we use concepts of graded exposure to get someone from needing a lot of sensory things, like lights on, windows locked, facing the window, eyes open to slowly getting people toward a little bit more safety. If that is not a possibility, finding another location and strategizing how we can prioritize our own safety and our own ability to relax rather than saying I must relax.
The other component of trauma in the course is the unveiling of how prevalent trauma is. In pelvic health, we talk a lot about sexual trauma because we are dealing a lot with the pelvic floor region and the genitals. One of the things I think we sometimes might be able to speak to more is the little subversive types of trauma. Whether it is emotional trauma, whether it is neglect, whether it is transgenerational trauma or intersectionality trauma…
There’s this other component in yoga that is coming out now that is the trauma that has been handed down through the yoga lineages. What I think is not understood is that a lot of people who practice yoga in a deep way have significant trauma from yoga. The question then is how do we reclaim a practice that is so lovely, done with care and kindness and non harming, for people who have maybe experienced it in a very harmful way – and introduce it as a non-harming, caring, compassionate method for people who haven’t experienced it. The whole idea is about how do you be in rest in your body and in empowerment.
Can you give an example of how a pelvic PT or OT would fit restorative yoga into their practice?
As PTs and Ots we are starting to bring mindfulness in, a lot, to our programming in terms of some of the work from Jon Kabat Zen on how great meditation is for so many things. There is still a question of “How do I put this in my plan of care?” The great thing about this class is that we can speak directly to this. Let's say that you are in a hospital-based scenario, you can give restorative yoga to someone n a hospital bed very easily. They’re not going anywhere and what a great thing to give them: a breathing practice, a concentration practice, and a rest practice.
For someone in private practice, such as orthopedics, this is the type of practice where maybe you’re not giving pelvic floor strengthening if someone has a large degree of overactivity in their pelvic floor. But they still need something to do at home, or they need something to do at the office. Maybe restorative yoga is a little bit too far out there for the patient. Maybe they don’t have a space they can lie down on the floor. That’s when we can say, ok how can we then transfer a pelvic floor restorative yoga posture to a desk situation? Can you cross your legs on your chair and lean forward, and modify it that way.
Then there is this component of the class that is all about breathing. I think we know in pelvic health how wonderful and how great breath-work can be and so some of these techniques can be used as ‘secret exercises’ in your everyday life in addition to being a dedicated practice. We talk about all of that in class.
Watch the full interview with Kate Bailey at the Herman & Wallace YouTube Channel:
Join Kate to learn more about including restorative yoga into your practice with Restorative Yoga for Physical Therapists this year. Courses are scheduled for:

Kate Bailey, PT, DPT, MS, E-RYT 500, YACEP, Y4C, CPI owns a private practice in Seattle that focuses on pelvic health for all genders and ages and works under a trauma-informed model where patient self-advocacy and embodiment are a priority. In addition to being a physical therapist, I’ve been teaching Pilates for nearly 20 years and yoga for over 10. Kate’s course, Restorative Yoga for Physical Therapists, combines live discussions and labs with pre-recorded lectures and practices that will be the basis for experiencing and integrating restorative yoga into physical therapy practice. Kate brings over 15 years of teaching movement experience to her physical therapy practice with specialties in Pilates and yoga with a focus on alignment and embodiment.
Yoga is a common term in our current society. We can find it in a variety of settings from dedicated studios, gyms, inside corporations, online, on Zoom, at home, and on retreat. The basic structure of a typical yoga class is a number of flowing or non-flowing postures, some requiring balance, some requiring going upside down, and many requiring significant mobility to achieve a certain shape. At the end of these classes is a pose called savasana, corpse pose (or sometimes translated for comfort as final resting pose). In this pose, which is often a treat for students after working through class, students lie on the ground, eyes closed, possibly supported by props, and rest. It is perhaps the only other time in the day when that person is instructed to lie on the floor in between sleep cycles.
Savasana is one of many restorative yoga postures. In the work created and popularized by Judith Hanson Lasater, PT, PhD1, restorative yoga has taken a turn away from the active physical postures, breath manipulations, and meditations that are commonplace in how we think of yoga. She has focused on rest and the need for rest in our current climate of productivity, poor self-care, and difficulty managing stress and pain.
In a dedicated restorative yoga class (not a fusion of exercise then rest, or stretch then rest… which are really lovely and have their own benefits), a student comes to class, gathers a number of props, and is instructed through 3 to 5 postures, all held for long durations to complete an hour or longer class. Consider what it would look like to do 3 things over one hour with the intent of resting. It is quite counter-culture. Students have various experiences with this type of practice, but over time many begin to feel the need for rest (or restorative practice) in a similar way that one feels thirsty or hungry.
We know the benefits of rest: being able to access the ventral vagal aspect of the parasympathetic nervous system is what Dr. Stephen Porges2 suggests supports health, growth, and restoration. There is the impact on the ventral vagal complex in the brainstem that regulates the heart, the muscles of the face and head, as well as the tone of the airway. To heal, we need access to this pathway. To manage stress, we need to access this pathway. To be able to choose our actions rather than be reactionary, we need to access this pathway. Restorative yoga is an accessible method that may be a new tool in a patient’s toolbox to help manage their nervous systems.
Join Kate Bailey to learn more about restorative yoga in Restorative Yoga for Physical Therapists this year. Courses are scheduled for:
1. Relax and Renew: Restful Yoga for Stressful Times by Judith Hanson Lasater PT, PhD
2. Polyvagal Theory by Stephen W Porges PhD


H&W is proud to be able to present a new remote course on ethics from new faculty member, and Sr. TA, Mora Pluchino, PT, DPT, PRPC. Mora is a graduate of Stockton University with a BS in Biology (2007) and Doctorate of Physical Therapy (2009). She has been working at Bacharach Institute for Rehabilitation ever since graduation and has experience in a variety of areas and settings, working with children and adults, including orthopedics, bracing, neuromuscular issues, vestibular issues, and robotics training.
Mora began treating Pelvic Health patients in 2016 and has experience treating women, men, and children with a variety of Pelvic Health dysfunction. In 2020, she opened her own "after hours" virtual practice called Practically Perfect Physical Therapy Consulting to help meet the needs of more clients and has been a guest lecturer for Rutgers University Blackwood Campus and Stockton University for their Pediatric and Pelvic Floor modules and has been a TA with Herman & Wallace since 2020 with over 150 hours of lab instruction experience. Mora authored and instructs Ethical Concerns for Pelvic Health Professionals.
● Your employer expects you to be responsible for supervising and billing for three orthopedic clients while you are in a private treatment area with a pelvic health patient. They say that you’re fine because the aide will be assisting the patients with their program.
● You are a new graduate, and your employer sends you to Pelvic Floor Level 1 and expects you to start up a Pelvic Health Program at the facility. Your first scheduled patient is a diagnosis you didn’t learn about and don’t feel comfortable treating, but your student loan payments have started, and you need this job.
● The word has gotten out and referrals are flowing into your clinic after hearing what a life-changing service your Pelvic Health program provides. You have a 6 month long waiting list and your front desk person asks you how to organize the list. Options include prioritizing based on the severity of issues, first come/ first serve, based on past history with the facility, etc.
Put yourself in these situations and reflect. How would you feel? What would you do? All of the situations above have a common theme. They present Ethical Concerns for Pelvic Health Professionals. Ethical situations are very common in day-to-day practice for any health care professional. Treating in the pelvic region can add additional complications due to the level of intimacy and vulnerability in this care.
Ethics by definition is “the division of philosophy concerned with how a person should behave in a matter that is considered morally correct or good” that gives us standards, virtues, and rules (Boone, 2017). The professional code of ethics for each professional category and is grounded in virtue ethics. Virtue ethics includes four main concepts including balance of harms and benefits, doing no harm, justice, and autonomy (Kirsch, 2005)
Whether a practitioner is a physical therapist/ physical therapist assistant, occupational therapist, psychologist, social worker, nurse, doctor, or physician’s assistant, their governing professional organization will have a code of ethics and conduct to help guide these practitioners in good decision making. There are many ethical decision-making models to help guide an individual through the process of identifying, defining, examining, and then problem solving any ethical occurrence.
The RIPS Model, originally presented by Arlanian, Swisher & Davis in 2005, presents an ethical framework to help guide practitioners through the steps needed to address ethical concerns. The world of ethical decision-making is typically one of many options, typically being more “gray area” than simply “black” and “white.” Ethical Concerns for Pelvic Health Professionals is designed to help make these decisions easier to define, examine, discuss, and address so we can have these tough conversations!
Ethical Concerns for Pelvic Health Professionals is a one-day remote course that covers ethical considerations for professionals working in the area of Pelvic Health. In general, Health Care Professionals have many day-to-day ethical considerations to “do no harm.” This includes basic decisions for billing, patient care, safety, and compliance. The purpose of this class is to explore the ethical challenges Pelvic Health practitioners may experience including consent, managing trauma and abuse, and preventing misconduct. To learn more join us in Ethical Concerns for Pelvic Health Professionals on June 18, 2022!
Research:
Boone, B. (2017). Ethics 101: From altruism and utilitarianism to bioethics and political ethics, an exploration of the concepts of right and wrong. Adams Media.
Kirsch, N. (2005). Ethics in Physical Therapy: A Case-Based Approach. McGraw Hill Publications. American Physical Therapy Association.

Kristina Koch, PT, DPT, is a board-certified women’s health physical therapist and certified lymphedema therapist who is the author/instructor of the remote course Pharmacologic Considerations for the Pelvic Health Provider. She has been treating pelvic health dysfunction in all ages and genders since 2001. Kristina works in private practice in Colorado Springs, CO, and has served as a guest lecturer for the pelvic health content at Regis University in Denver and the University of Colorado.
Did you know that the median length of time a primary care provider spends with a patient is 15 minutes? This breaks down to approximately 5 minutes for the patient to talk about their health concerns and 5 minutes for the health care provider to speak, with the rest being applied toward paperwork (1). After this appointment, the patient may not be seen again for several months or even a year. Medication side effects that impact the patients’ quality of life, or create new symptoms, can be easily overlooked.
I created the course, Pharmacologic Considerations for the Pelvic Health Provider because, with direct access to physical and occupational therapy services, a greater responsibility has been placed upon the therapist to take on more of a role as a primary care provider. We must ensure that all factors contributing to a patient’s signs and symptoms are considered. This includes reviewing and assessing if medications or supplements may be causative.
As therapists, we typically spend more time with our patients than their primary care providers. We are seeing them for longer periods during a treatment session and will see them numerous times throughout a month or longer. As a result, our patients have a greater opportunity to discuss their signs and symptoms with us versus their physician or primary care provider. Therefore, understanding how medications may be impacting a patient is essential. Being able to educate the patient about the side effects of the medications they are taking and how the medications may be contributing to their complaints can enhance the value of the treatment session.
By possessing this knowledge and understanding of the medications that are prescribed to treat pelvic health, therapists can have educated conversations with our patients and other health care providers involved in their care. The ability to discuss the most recent medications and supplements or complementary alternatives, that may minimize side effects or have fewer impacts on quality of life and enhance function, is an integral part of patient care.
Join Kristina to dive into Pharmacologic Considerations for the Pelvic Health Provider. This one-day, virtual course will discuss the importance of understanding pharmacology and review commonly prescribed medications. Kristina also spends time explaining current research pertaining to the pharmacologic treatment of numerous pelvic and reproductive health conditions, medication side effects, drug interactions, and non-pharmacologic alternatives. Medications discussed include those for constipation and GI dysfunction, pelvic pain conditions (including vulvodynia, chronic prostatitis, and endometriosis), as well as medications and side effects in Gender-Affirming Care for patients who are transitioning.
Upcoming 2022 course dates for Pharmacologic Considerations for the Pelvic Health Provider include:
References:
- Tai-Seale, M., McGuire, T. G., & Zhang, W. (2007). Time allocation in primary care office visits. Health Services Research. 42(5), 1871-1894. Doi:10.1111/j.175-6773.2006.00689.x
- Ciccone, C. D. (2007). Pharmacology in Rehabilitation. (4th). F.A. Davis Company.

This week the interviewer becomes the interviewee as Stacey Futterman Tauriello sits down to interview Holly Tanner on the Male Pelvic Floor course.
Stacey Futterman reached out to Holly Tanner back in 2007 through a phone call to see if they could partner on a lecture covering male pelvic pain. The two had never met in person but decided to collaborate on the three-hour APTA National Conference lecture. Holly shares "I still recall the frequent glances I made to match the person behind the voice I had heard for so many long phone calls.”
This presentation was developed into a two-day education course for Herman & Wallace and contained lectures on male anatomy, post-prostatectomy urinary incontinence, pelvic pain, and sexual health and dysfunction. The big question of the time was “should we allow men to attend?” Holly puts this in perspective, “As strange as this question now seems, it speaks volumes about the world of pelvic health at that time; mostly female instructors taught mostly female participants about mostly female conditions.”
The Male Pelvic Floor course was first taught in 2008 and has since been expanded to include 22 contact hours. This current content includes 7 pre-recorded lectures and 2 full days of live lectures and labs, allowing more time for hands-on skills in examination and treatment. The schedule still covers bladder, prostate, sexual health, and pelvic pain, and further discusses special topics like post-vasectomy syndrome, circumcision, and Peyronie’s disease.
Because the course often has providers in attendance who have not completed prior pelvic health training, instruction in basic techniques is included. For the experienced therapists, there are multiple lab “tracks” that offer intermediate to advanced skills that can be practiced in addition to the basic skills. Holly adds, “One of the more valuable conversations that we have in the course is how to create comfort and ease in when for most us, we were raised in a culture (and medical training) where palpation of the pelvis was not made comfortable. Hearing from the male participants about their bodies, how they are affected by cultural expectations, adds significant value as well.”
In 2017 Herman & Wallace faculty member, Heather Radar submitted a blog where she wrote about a note that was left on her doorstep by the wife of an older gentleman who had chronic male pelvic pain. When looking into writing this blog I kept coming back to this past blog by Heather, and I have decided to share an abridged version today to accompany Holly Tanner's short interview discussing the Male Pelvic Floor Satellite Lab Course.
Recently, a note was left at my doorstep by the wife of an older gentleman who had chronic male pelvic pain. His pain was so severe, that he could not sit, and he lay in the back seat of their idling car as his wife, having exhausted all other medical channels available to her, walked this note up to the home of a rumored pelvic floor physical therapist who also treated men. The note opened with how she had heard of me. She then asked me to contact her about her husband’s medical problem. It ended with three words that have vexed me ever since…we are desperate. We Are Desperate.
Unlike so many men with chronic pelvic pain, he had at least been given a diagnostic cause of his pain, pelvic floor muscle dysfunction, rather than vaguely being told it was just a prostate issue. However, the therapists that had been recommended by his doctor only treated female pelvic dysfunction.
My first thought after reading the note was, “I bet shoulder or knee therapists don’t get notes like this on their doorstep.” My next thought, complete with facepalm, “THIS HAS TO STOP! Pelvic floor rehab has got to become more accessible”.
Pelvic floor therapists see all people including men, women, and transgender. They treat the pediatric, adult, and geriatric populations. They treat pelvic floor disorders in the outpatient, home health, and SNF settings. They treat elite athletes and those with multiple co-morbidities using walkers. They can develop preventative pelvic wellness programs and teach caregivers how to better manage their loved one’s incontinence. This is due to one simple fact: No matter the age, gender, level of health, or practice setting, every patient has a pelvic floor.
The pelvic floor should not be regarded as some rare zebra in clinical practice when it is the workhorse upon which so many health conditions ride. It interacts with the spine, the hip, the diaphragm, and vital organs. It is composed of skin, nerves, muscles, tendons, bones, ligaments, lymph glands, and vessels. It is as complex and as vital to function and health as the shoulder or knee is, and yet students are lucky if they get a “pelvic floor day” in their PT or OT school coursework.
I call for every therapist, specialist, and educator to learn more about the pelvic floor. If you only treat pelvic dysfunction in women, please consider expanding your specialty to include men. The guys really need your help. You literally may be the only practitioner around that has the skills to treat these types of problems. Yes, the concerns you have about privacy and feeling comfortable are valid. But, you are not alone in this. Smart people like Holly Tanner have figured all that stuff out for you and can guide you on how to expertly treat in the men’s health arena.
The Silver Lining. Thanks to the champions of pelvic floor rehab education, we’ve come a long way. The good news in this story is that this man’s doctor recognized early that he had pelvic floor muscle dysfunction and recommended that he see a pelvic floor physical therapist. The bad news-it took 2 years before he could find one. The ball is in our court, therapists. Let’s do better. Until there are no more men in the back seat, we still need to #LearnMoreAboutThePelvicFloor.
We need to continue to create more coursework and more clinical training opportunities so that the representation of those treating male patients improves. If you feel ready to take your training to the next level in caring for male pelvic dysfunction, join us for an upcoming Male Pelvic Floor Satellite Lab Course.

Male Pelvic Floor Satellite Lab Course is scheduled on several dates and satellite locations for 2022, including self-hosted course options. Dates include:
- April 23-24
- June 12-13
- September 24-25
- October 22-23
- December 3-4


Blog by Deanna Vaughn, PT, DPT who practices at Core and Pelvic Physical Therapy Clinic in Conway, Arkansas, this article was originally located at https://whatsupdownthere.info/colorectal-cancer-the-gut-and-the-butt/.
Colorectal cancer refers to cancerous cells within the colon or rectum. Need a quick anatomy review? Keep reading then!
The colon is another name for the large intestine, which is the long tube (nearly 5 FEET!) surrounding the small intestines (that snaky, jumbled tube in the middle of our bodies, which you can see below in the picture). It’s comprised of segments: the cecum (the little pouch that joins the small intestine to the large intestine) in the right lower abdomen, the ascending colon starting at the right lower part of your abdomen (coming off the cecum), and up to about the right side of your ribcage; the transverse colon that loops underneath the stomach and ribcage from right to left; the descending colon that extends down from the left side of your ribcage to the lower part of your left abdomen; and then the sigmoid colon that loops (in an s-shape) along the lower abdomen to the center of the body. At the end of the colon is the rectum, which pretty much connects the colon to the actual anus/anal opening for wastes to leave the body.
That being said, colorectal cancer can affect any part or segment of the colon and the rectum. If you have a family history of colorectal cancer, or if you have an inflammatory bowel disease (like Crohn’s disease or ulcerative colitis), then you may be at a higher risk for colorectal cancer. Other risk factors are the same for virtually any other health condition – genetics, no regular physical activity, poor diet, tobacco use, high alcohol consumption, etc.
So how would we know if it’s colorectal cancer – or precancerous cells, and how do we decrease our risk?
That’s where screening comes into play! Just like how someone may see their gynecologist annually and undergo the PAP smear every 1-3 years to check for any gynecological cancer (like cervical or labial cancer), someone may see their colorectal or gastrointestinal (GI) provider to check for colorectal cancer or disorders. Regular screening takes place around age 45 (although a person may be screened earlier if they are at higher risk or had a previous history of cancer).
What does screening look like?
There are a few tests that screen for colorectal cancer. These tests include stool tests, flexible sigmoidoscopy, and colonoscopy.
Stool tests – This pretty much involves you taking a sample of your stool via test kit provided to you, and returning it to your doctor/lab, where your stool is checked for any blood or other abnormal findings.
Flexible sigmoidoscopy – A thin, short tube with a light is inserted into the rectum. This allows your doctor to see any polyps or cancer within the rectum and lower part of the colon.
Colonoscopy – This is like the sigmoidoscopy, but with a longer tube. The longer tube allows your doctor to check for polyps/cancer inside the rectum and the entire length of the colon. Your doctor can also remove some polyps during this procedure if indicated.
Most people without any symptoms, abnormal findings or outstanding personal or family history of colorectal cancer will have these screening tests performed anywhere from 5-10 years.
What are the symptoms?
This is not an exhaustive list, but some symptoms may include:
- Bleeding, pain, and/or discomfort within the rectum/anus
- Blood in stool
- Abdominal pain and bloating
- Nausea/vomiting
- Difficulty or incomplete bowel evacuation
- Hemorrhoids
- Altered bowel habits (such as sudden constipation, diarrhea, change in stool consistency)
Now what are our treatment options?
Besides preventative measures – such as getting regular physical activity, improving our diet, etc., treatment looks similar to any other cancer treatment. This may look like chemotherapy, radiation therapy, immunotherapy, and/or surgery. Surgery may be indicated to remove polyps/tumors, or parts of the colon or rectum to eliminate cancerous growths. Thankfully though, regular screening of the colorectal region can find precancerous/cancerous cells early. Oftentimes, such as during a colonoscopy, your colorectal provider may go ahead and remove polyps that are abnormal or deemed precancerous at that time!
Now what about pelvic physical therapy? Can it possibly help?
Well, this is another condition (like Pelvic Congestion Syndrome in the previous blog post), where pelvic physical therapy is not the initial go-to or main treatment option. Individuals with colorectal cancer vary in several ways depending on staging/severity and overall health. Once again, pelvic therapy is a nice resource to utilize if you’re needing or wanting ways to manage your bowel symptoms.
Ways that pelvic PT CAN help may include: Teaching appropriate toileting – positioning to straighten out the anorectal angle and allow stool to pass more easily from the rectum; mechanics, such as exhaling smoothly when pushing for a bowel movement to prevent straining; Improving pelvic floor muscle function (strength, endurance, coordination) so that your body can delay defecation as needed and calm down bowel urges; and overall promoting health bowel habits by supporting your nutrition and keeping bowel movements regular.
Whether or not you (or someone you know) have colorectal cancer, developing healthy and safe bowel habits is key to a better quality of life. Working with your doctor and/or your team of providers is important in making sure your needs are addressed, but feel free to reach out to your local pelvic PT if you want more resources or guidance – even things like, “So, how SHOULD I be pooping??”
References & Resources
Brenner H, Chen C. The colorectal cancer epidemic: challenges and opportunities for primary, secondary and tertiary prevention. Br J Cancer. 2018;119(7):785-792. doi:10.1038/s41416-018-0264-x
https://www.cancer.org/cancer/colon-rectal-cancer.html
https://my.clevelandclinic.org/health/diseases/14501-colorectal-colon-cancer
Kuipers EJ, Grady WM, Lieberman D, et al. Colorectal cancer. Nat Rev Dis Primers. 2015;1:15065. Published 2015 Nov 5. doi:10.1038/nrdp.2015.65
Leslie A, Steele RJC. Management of colorectal cancerPostgraduate Medical Journal 2002;78:473-478. http://dx.doi.org/10.1136/pmj.78.922.473
Mármol I, Sánchez-de-Diego C, Pradilla Dieste A, Cerrada E, Rodriguez Yoldi MJ. Colorectal Carcinoma: A General Overview and Future Perspectives in Colorectal Cancer. Int J Mol Sci. 2017;18(1):197. Published 2017 Jan 19. doi:10.3390/ijms18010197
You YN, Lee LD, Deschner BW, Shibata D. Colorectal Cancer in the Adolescent and Young Adult Population. JCO Oncol Pract. 2020;16(1):19-27. doi:10.1200/JOP.19.00153

Dawn Sandalcidi PT, RCMT, BCB-PMD is known as the go-to expert in the field of pediatric pelvic health. She has been practicing for 40 years this May and has concentrated on the pediatric pelvic floor for 29 of those. When it comes to pediatric pelvic floor issues, there is so much more than bedwetting, and often the practitioner needs to look beyond the pelvic floor.
Despite the growing number of pelvic rehab specialists treating men and women with PF dysfunction, children in this patient population remain woefully under-served. This can cause undue stress for the child and family, as well as the development of internalizing and externalizing psychological behaviors. Many of the techniques used in pediatric pelvic therapy can be translated to the adult population. The question is ‘who’s the driver?’ In pediatrics, it is typically a bowel issue.
The Standard American Diet involves food that is high in calories, saturated fats, trans fats, added sugars, and sodium. It is also lacking in the intake of essential nutrients for the body like fiber, calcium, potassium, and vitamin D. This lack of dietary fiber can cause issues with the digestive tract as well as the colon leading to constipation. Bowel dysfunction including constipation can contribute to urinary leakage and urgency (1). Constipation accounts for approximately 5% of visits to pediatric clinics (2) proving that there is a need for practitioners to know how to treat these pediatric issues.
Dawn focuses much of her pediatric knowledge on her two courses: Pediatric Incontinence and Pelvic Floor Dysfunction (PEDs) and Pediatric Gastrointestinal Disorders (PEDsG). Pediatric pelvic floor basics are covered in PEDs, including instruction in anatomy, physiology, development of normal voiding reflexes and urinary control, and learning how to talk with child patients. Biofeedback and ultrasound (which Dawn fondly calls jelly belly) are also covered and can be helpful as less invasive procedures for children.
PEDsG goes beyond the pelvic floor and opens up the door to look at the big picture of the whole child. Dawn shares that almost 80% of her kiddos with chronic constipation present with diastasis rectus abdominus. They can also have hyperextension in the thoracic spine, and the rib cage is postally rotated – where the kids don’t know how to bring it down.
Dawn is also on the threshold of writing a pediatric pelvic pain course that she expects to be ready later this year. Pediatric pelvic pain is becoming more prevalent, and it can’t be treated the same way as in adults. Dawn explains that “children don’t understand, so we’re actually creating a pediatric pain neuroscience protocol. It is a bio-psycho-social approach, and we use fun things.”
Research tells us that 15% of kids per year will outgrow bedwetting. Children who suffer from bedwetting can feel ashamed and embarrassed, have self-esteem issues, or even act out. There are 5 basics of where you start with a pediatric patient that are taught in PEDs. Dawn also shares 5 basics in her e-book, BEDWETTING BOOTCAMP(3):
- Avoid things that can irritate the bladder
- Avoid drinking anything just before bed
- Drink throughout the day
- Empty your bladder throughout the day
- Avoid constipation and straining
Everything in Pediatric Incontinence and Pelvic Floor Dysfunction builds into Pediatric Gastrointestinal Disorders, and everything in PEDsG builds into Pediatric Pelvic Pain. The more practitioners who learn about the pediatric pelvic floor means that more kids get treated and the fewer adults that will have pelvic floor dysfunction. To learn more about treating pediatric pelvic health register for one of Dawn Sandalcidi’s upcoming courses:
Pediatric Incontinence and Pelvic Floor Dysfunction: August 27-28th
Pediatric Gastrointestinal Disorders: May 14-15, November 12-13
References:
- Sandalcidi (Spring 2018). Paediatric incontinence and pelvic floor dysfunction. Journal of Pelvic, Obstetric and Gynaecological Physiotherapy, 122, 5–8.
- Thibodeau B. A., Metcalfe P., Koop P. & Moore K. (2013) Urinary incontinence and quality of life in children. Journal of Pediatric Urology 9 (1), 78–83.
- Dawn Sandalcidi PT, RCMT, BCB-PMD. BEDWETTING BOOTCAMP Frustrated by Bed Wetting? The 5 Ways to Speed Starting Up Dry Tonight! www.kidsbowelbladderPMD.com. https://cdn.fs.teachablecdn.com/YfP5rUfiRtOJxXZSZUso
All Upcoming Continuing Education Courses

Pelvic Function Level 1 - Satellite - Milwaukee WI - July 12 - 13 2025 - SOLD OUT
Jul 12 2025 - Jul 13 2025

Modalities and Pelvic Function - In-Person - Houston TX - July 12 - 13 2025
Jul 12 2025 - Jul 13 2025

Pelvic Function Level 1 - Satellite - Denver CO - July 12 - 13 2025 - SOLD OUT
Jul 12 2025 - Jul 13 2025




Pelvic Function Level 1 - Satellite - Des Moines IA - July 26 - 27 2025 - SOLD OUT
Jul 26 2025 - Jul 27 2025

Pelvic Function Level 1 - Satellite - Minneapolis MN - July 26 - 27 2025 - SOLD OUT
Jul 26 2025 - Jul 27 2025

Pelvic Function Level 1 - Satellite - Paso Robles CA - July 26 - 27 2025 - SOLD OUT
Jul 26 2025 - Jul 27 2025

Pelvic Function Level 1 - Satellite - St. Augustine FL - July 26 - 27 2025
Jul 26 2025 - Jul 27 2025

Pelvic Function Level 1 - Satellite - Virginia Beach VA - July 26 - 27 2025 - SOLD OUT
Jul 26 2025 - Jul 27 2025


Pelvic Function Level 1 - In-Person - Chicago IL - August 2 - 3 2025 - SOLD OUT
Aug 2 2025 - Aug 3 2025



Menopause Transitions and Pelvic Rehab - Remote Course - August 9 - 10 2025
Aug 9 2025 - Aug 10 2025









Pelvic Function Level 2C - Satellite - Palm Beach FL - August 16 - 17 2025
Aug 16 2025 - Aug 17 2025

Pelvic Function Level 2C - Satellite - New Orleans LA - August 16 - 17 2025
Aug 16 2025 - Aug 17 2025
Pelvic Function Level 2C - Satellite - Paso Robles CA - August 16 - 17 2025
Aug 16 2025 - Aug 17 2025


Pediatrics Level 1 - Treatment of Bowel and Bladder Disorders - Remote Course - August 23 - 24 2025
Aug 23 2025 - Aug 24 2025

Pelvic Function Level 1 - Satellite - Jacksonville FL - August 23 - 24 2025
Aug 23 2025 - Aug 24 2025

Pelvic Function Level 1 - Satellite - Chicago IL - August 23 - 24 2025 - SOLD OUT
Aug 23 2025 - Aug 24 2025


Pelvic Function Level 1 - Satellite - Hermosa Beach CA - August 23 - 24 2025
Aug 23 2025 - Aug 24 2025

Rehabilitative Ultrasound Imaging Pelvic Health Satellite Lab Course - Self-Hosted - September 5 - 7 2025
Sep 5 2025 - Sep 7 2025
Rehabilitative Ultrasound: Orthopedic Topics Satellite Lab Course - Self-Hosted - September 5 - 6 2025
Sep 5 2025 - Sep 6 2025

Rehabilitative Ultrasound Imaging Pelvic Health Satellite Lab Course - Indianapolis IN - September 5 - 7 2025
Sep 5 2025 - Sep 7 2025
